Prurigo pigmentosa: Report of two cases in the United States and review of the literature
Published Web Location
https://doi.org/10.5070/D36rv324m4Main Content
Prurigo pigmentosa: Report of two cases in the United States and review of the literature
Talley Whang MD, A Yasmine Kirkorian MD, Anna Krishtul MD, Robert Phelps MD, Helen Shim-Chang MD
Dermatology Online Journal 17 (12): 2
Mount Sinai School of Medicine, New York, New YorkAbstract
Prurigo pigmentosa is a rare inflammatory skin disease of unknown etiology that presents as a pruritic truncal eruption of reticulated and symmetric macules and papules with the predilection for young Japanese females. Although cases of PP are increasingly reported in the non-Japanese literature, dermatologists may be unfamiliar with this entity. Here we report two American women, one Caucasian and one of Chinese descent, with PP and present a discussion of the literature. The treatments of choice for prurigo pigmentosa are tetracyclines such as doxycycline and minocycline, as well as dapsone. The prognosis is excellent.
Case 1
A 35-year-old woman presented with a 2-year history of a recurrent, pruritic eruption on the upper back. Her medical and family histories were unremarkable. Prior to presenting to our department, the patient underwent several skin biopsies and she was incorrectly diagnosed with recurrent herpes simplex virus (HSV) infection despite negative viral cultures. At that time, she was treated with anti-HSV therapy (oral acyclovir, oral valcyclovir, and topical acyclovir ointment) and topical steroids with no improvement in her condition. Laboratory studies, including complete blood count, comprehensive metabolic panel, urinalysis, urine porphyrins, and anti-Ro/La and anti-5S RNA/protein antibodies, were within normal limits. The anti-nuclear antibody titer was 1:160. Anti-double stranded DNA and anti-Smith antibodies were negative. The patient denied experiencing typical malar rash, discoid lesions or mucosal ulcers. She denied any joint pains, pleuritic chest pain, or neurologic deficits such as seizures or psychosis. Her renal function was within normal limits as demonstrated by normal creatinine and urinalysis. Based on these results and the lack of characteristic signs and symptoms, lupus erythematosus was ruled out in this patient. Patch testing revealed a 1+ reaction to cobalt and neomycin, which were thought to not be clinically relevant given no history of exposure. Minimal erythema dose testing to UVA and UVB were within normal limits.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Patient 1: Multiple erythematous papules and vesicles, some crusted, interspersed among light brown hyperpigmented
macules coalescing in a reticular pattern on the upper back. Figure 2. Biopsy of patient 1: Focal necrosis, intraepidermal vesiculation, and prominent dermal lymphoid infiltrate representative of a fully developed lesion of prurigo pigmentosa | |
 |
| Figure 3 |
|---|
| Figure 3. Patient 1: Resolution with post-inflammatory macules and patches after minocycline therapy |
Physical exam revealed multiple erythematous papules, vesicles, and excoriated crusts in the acute stage, interspersed among light brown hyperpigmented macules coalescing into patches on the upper back and on the nape of the neck (Figure 1). Skin biopsy demonstrated focal necrosis, intraepidermial vesiculation, and a prominent lymphoid infiltrate in the dermis (Figure 2). The patient was treated with minocycline 100 mg daily for 3 weeks with rapid resolution of pruritis and cessation of new lesions, leaving behind just reticulated hyperpigmentation (Figure 3). The clinical history, biopsy results, and dramatic response to minocycline therapy led to the diagnosis of PP.
Case 2
A 21-year-old woman of Chinese descent presented with a 3-year history of intermittently pruritic rash involving the entire back. She had no significant medical history. The patient had been treated for presumed eczema with various topical corticosteroids as well as pulses of oral prednisone with little relief.
 |  |
| Figure 4 | Figure 5 |
|---|---|
| Figure 4. Patient 2: Symmetrically distributed erythematous macules and papules in a reticular pattern surrounding central
hyperpigmented patches Figure 5. Patient 2: A close-up of peripherally located erythematous and scaly papules | |
Physical exam was strikingly similar to that of Patient #1. Like the previous case, this patient had erythematous macules and papules symmetrically distributed in a reticulated pattern on the back, with active lesions on the periphery, and light-brown macules and patches in the center (Figures 4 and 5). Skin biopsy of an erythematous scaly papule on the edge demonstrated superficial perivascular mixed infiltrate with spongiosis and collections of neutrophils in the epidermis. Some necrotic keratinocytes as well as scale-crust were also observed (Figure 6). The clinical presentation and biopsy led to the diagnosis of PP and the patient was treated with minocycline 100 mg daily for two weeks, resulting in complete resolution of pruritus and erythema. At 10 months post-treatment, the patient had no recurrence of symptoms; only post-inflammatory reticulated hyperpigmented patches remained on her back.
 |  |
| Figure 6 | Figure 7 |
|---|---|
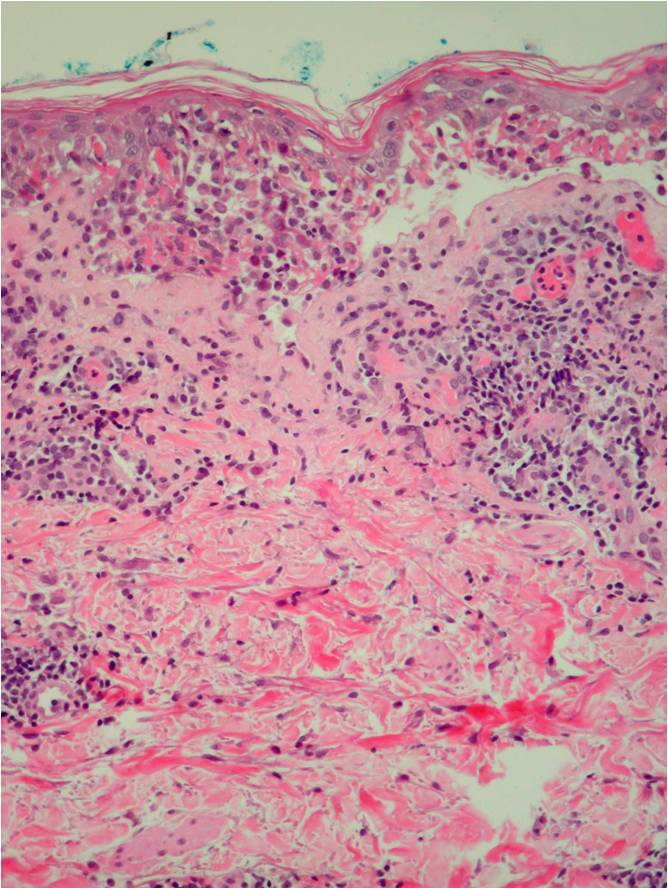
| Figure 6. Biopsy of patient 2: Superficial perivascular mixed infiltrate with spongiosis and collections of neutrophils in
the epidermis, consistent with an early lesion of prurigo pigmentosa Figure 7. Biopsy of patient 2. In this early lesion of PP, some necrotic keratinocytes as well as scale-crust are observed. | |
Discussion
In 1971, Nagashima et al. first described their observation of eight patients with “a peculiar pruriginous dermatosis with gross reticular pigmentation” and suggested the name “prurigo pigmentosa” for this condition [1]. Following this initial description, more than 300 patients with prurigo pigmentosa (PP) have been described in the Japanese literature [2]. However, fewer than 50 cases have been reported in non-Japanese patients and only 3 cases have been reported in the United States [3, 4, 5].
Prurigo pigmentosa presents as a recurrent, pruritic eruption of erythematous macules and papules symmetrically distributed on the trunk with a predilection for the upper back, sacrum, abdomen, chest [6], and more rarely, the limbs or face [7]. There are no reports of involvement of the mucous membranes, hair, or nails. Vesicular and bullous forms of PP have been reported [8-12]. Patients may present with episodes that recur over a period of months to years, which upon resolution, leave behind a pattern of reticulated or mottled hyperpigmentation. This entity is seen more commonly in young females. Ackerman et al reported a mean age at time of diagnosis of 25 and a female to male ratio of 2:1 [6]. Our patients were young females presenting with the typical eruption on the upper back and nape of the neck, recurring over a 2-3 year period.
Although the pathogenesis of PP remains elusive, associations with systemic conditions including atopy [13, 14], Helicobacter pylori infection [15], Sjogren syndrome, and adult-onset Still disease have been reported [16, 17]. More recently, Park et al. [18] have reported 3 patients with PP who had elevated anti-nuclear antibody titers. Similar to our first patient, these patients did not have any antibodies that are more specific to lupus erythematosus. In addition, they did not have any physical signs or symptoms diagnostic of lupus. Although elevated ANA titers are a non-specific finding that can be present in up to 20 percent of the normal population, the authors suggest that autoimmunity may play a role in the pathogenesis of PP.
The presence of a neutrophilic infiltrate early and a lymphocytic infiltrate late in the disease suggests a reactive process. To this end, certain case reports have suggested a reaction to various allergens, including trichlorphenol [19], chromium in acupuncture needles [20], chrome in detergent [21], and nickel [22]; a contact allergy to clothing has also been suggested [23]. However, the majority of patients do not have a history of exposure to an allergen. Our first case had a 1+ reaction to cobalt and neomycin on patch testing, but these allergens did not seem to play a role in the pathogenesis of her condition.
Another notable association frequently reported in the literature is with ketosis resulting from diabetes [10, 24-29], diet [30, 31, 32], eating disorders [33, 34], or pregnancy [35]. Although several authors have reported improvement of the eruption upon resolution of ketosis [25], there is no noted association with blood glucose levels [29]. Patient #1 had normal levels of blood glucose and no evidence of elevated ketones. Although Patient #2 was not tested, there were no clinical signs or symptoms to suspect abnormalities of serum glucose or ketones.
Despite the unclear etiology, Ackerman et al. have described a distinct histopathologic sequence in the lesions of PP [6]. Early lesions demonstrate a superficial perivascular neutrophilic infiltrate with papillary dermal edema, spongiosis, collections of neutrophils in the epidermis, and a few necrotic keratinocytes. In a fully developed lesion, there is a patchy lichenoid infiltrate in which lymphocytes predominate, with spongiosis intra- and subepidermal vesiculation and numerous necrotic keratinocytes. Finally, the late lesion demonstrates a lymphocytic infiltrate, mild epidermal hyperplasia, parakeratosis, scale-crust, and few to many melanophages. The lesions are negative on direct immunofluorescence. Based on this observation, the biopsy from Patient #1 represented a fully developed lesion of PP and that from Patient #2 showed an early lesion.
The significance of the early neutrophilic infiltrate in the pathogenesis of PP is supported by the efficacy of the two drugs most commonly used to treat this condition: minocycline and dapsone. These agents are known to block neutrophil chemotaxis and function [36-41]. In addition to tetracycline derivatives [6, 10, 12, 14, 31, 37, 41-52] and dapsone [4, 5, 28, 53] patients have been treated with macrolide antibiotics [15, 54] and isotretinoin [8, 55]. Topical steroids are not effective in the treatment of PP. Both of our patients were successfully treated with minocycline 100 mg/day for 2 to 3 weeks with resolution of lesions and no recurrence to date (Length of follow up: Patient #1: 3 years, Patient #2: 10 months)
Despite the distinctive clinical and histopathological presentation, the diagnosis of prurigo pigmentosa can remain elusive because practitioners may be unfamiliar with the clinical and histopathological characteristics of this rare inflammatory disorder. Dermatologists are urged to suspect prurigo pigmentosa when a patient presents with a reticulated pruritic eruption on the trunk that is not relieved by empiric treatment with topical steroids.
References
1. Nagashima M, Ohshiro A, Shimizu N. A peculiar pruriginous dermatosis with gross reticular pigmentation. Jap J Dermatol 1971;81:38-9. [PubMed]2. Teraki Y, Nishikawa T. Skin diseases described in Japan 2004. J Dtsch Dermatol Ges 2005 Jan;3(1):9-25. [PubMed]
3. Dijkstra JW, Bergfeld WF, Taylor JS, Ranchoff RE. Prurigo pigmentosa. A persistent lichenoid reaction to bismuth? Int J Dermatol 1987 Jul-Aug;26(6):379-81. [PubMed]
4. Joyce AP, Horn TD, Anhalt GJ. Prurigo pigmentosa. report of a case and review of the literature. Arch Dermatol 1989 Nov;125(11):1551-4. [PubMed]
5. Roehr P, Paller AS. A pruritic eruption with reticular pigmentation. Prurigo pigmentosa. Arch Dermatol. 1993;129:365-370. [PubMed]
6. Boer A, Misago N, Wolter M, Kiryu H, Wang XD, Ackerman AB. Prurigo pigmentosa: A distinctive inflammatory disease of the skin. Am J Dermatopathol 2003 Apr;25(2):117-29. [PubMed]
7. Miyakawa S, Kurihara S, Nishikawa T. Prurigo pigmentosa affecting the forehead. Dermatologica 1984;169(3):135-7. [PubMed]
8. Requena Caballero C, Nagore E, Sanmartin O, Botella-Estrada R, Serra C, Guillen C. Vesiculous prurigo pigmentosa in a 13-year-old girl: Good response to isotretinoin. J Eur Acad Dermatol Venereol 2005 Jul;19(4):474-6. [PubMed]
9. Matsumoto C, Kinoshita M, Baba S, Suzuki H, Kanematsu S, Kanematsu N. Vesicular prurigo pigmentosa cured by minocycline. J Eur Acad Dermatol Venereol 2001 Jul;15(4):354-6. [PubMed]
10. Kubota Y, Koga T, Nakayama J. Bullous prurigo pigmentosa and diabetes. Eur J Dermatol 1998 Sep;8(6):439-41. [PubMed]
11. Kim SK, Kang HY, Lee ES. Bullous prurigo pigmentosa. Int J Dermatol 2007 Aug;46(8):888-90. [PubMed]
12. De Francesco V, Quinkenstein E, Mariuzzi L, Frattasio A, Pillon B, Patrone P. Bullous prurigo pigmentosa. Eur J Dermatol 2006 Mar-Apr;16(2):184-6. [PubMed]
13. Kwon HJ, Kim MY, Kim HO, Park YM. Two cases of prurigo pigmentosa in atopic patients. J Dermatol 2006 Aug;33(8):579-82. [PubMed]
14. Cota C, Donati P, Amantea A. Prurigo pigmentosa associated with an atopic diathesis in a 13-year-old girl. Pediatr Dermatol 2007 May-Jun;24(3):277-9. [PubMed]
15. Erbagci Z. Prurigo pigmentosa in association with helicobacter pylori infection in a caucasian turkish woman. Acta Derm Venereol 2002;82(4):302-3. [PubMed]
16. Tomaru K, Nagai Y, Ohyama N, Hasegawa M, Endo Y, Tamura A, Ishikawa O. Adult-onset still's disease with prurigo pigmentosa-like skin eruption. J Dermatol 2006 Jan;33(1):55-8. [PubMed]
17. Togawa Y, Shinkai H, Utani A. Prurigo pigmentosa in a patient with primary biliary cirrhosis and sjogren syndrome. J Dermatol 2004 Oct;31(10):815-9. [PubMed]
18. Park HY, Hong SP, Ahn SY, Ji JH, Choi EH, Jeon SY. Antinuclear antibodies in patients with prurigo pigmentosa: a linkage or a coincidence? Dermatology 2009;218:90-91. [PubMed]
19. Cotterill JA, Ryatt KS, Greenwood R. Prurigo pigmentosa. Br J Dermatol 1981 Dec;105(6):707-10. [PubMed]
20. Tanii T, Kono T, Katoh J, Mizuno N, Fukuda M, Hamada T. A case of prurigo pigmentosa considered to be contact allergy to chromium in an acupuncture needle. Acta Derm Venereol 1991;71(1):66-7. [PubMed]
21. Kim MH, Choi YW, Choi HY, Myung KB. Prurigo pigmentosa from contact allergy to chrome in detergent. Contact Dermatitis 2001 May;44(5):289-92. [PubMed]
22. Atasoy M, Timur H, Arslan R, Ozdemir S, Gursan N, Erdem T. Prurigo pigmentosa in a patient with nickel sensitivity. J Eur Acad Dermatol Venereol 2008 May 21. [PubMed]
23. Yamasaki R, Dekio S, Moriyasu S, Takagaki K. Three cases of prurigo pigmentosa. J Dermatol 1981;8:125-132. [PubMed]
24. Kobayashi T, Kawada A, Hiruma M, Ishibashi A, Aoki A. Prurigo pigmentosa, ketonemia and diabetes mellitus. Dermatology 1996;192(1):78-80. [PubMed]
25. Ohnishi T, Kisa H, Ogata E, Watanabe S. Prurigo pigmentosa associated with diabetic ketoacidosis. Acta Derm Venereol 2000 Nov-Dec;80(6):447-8. [PubMed]
26. Yokozeki M, Watanabe J, Hotsubo T, Matsumura T. Prurigo pigmentosa disappeared following improvement of diabetic ketosis by insulin. J Dermatol 2003 Mar;30(3):257-8. [PubMed]
27. Murao K, Urano Y, Uchida N, Arase S. Prurigo pigmentosa associated with ketosis. Br J Dermatol 1996 Feb;134(2):379-81. [PubMed]
28. Teraki Y, Teraki E, Kawashima M, Nagashima M, Shiohara T. Ketosis is involved in the origin of prurigo pigmentosa. J Am Acad Dermatol 1996 Mar;34(3):509-11. [PubMed]
29. Courtois JM, Dalac S, Collet E, Ladurelle AS, Lambert D. Prurigo pigmentosa. Ann Dermatol Venereol 1992;119(10):757-9. [PubMed]
30. Gur-Toy G, Gungor E, Artuz F, Aksoy F, Alli N. Prurigo pigmentosa. Int J Dermatol 2002 May;41(5):288-91. [PubMed]
31. Mitsuhashi Y, Suzuki N, Kawaguchi M, Kondo S. Prurigo pigmentosa on a patient with soft-drink ketosis. J Dermatol 2005 Sep;32(9):767-8. [PubMed]
32. Nakada T, Sueki H, Iijima M. Prurigo pigmentosa (nagashima) associated with anorexia nervosa. Clin Exp Dermatol 1998 Jan;23(1):25-7. [PubMed]
33. Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol 2005;6(3):165-73. [PubMed]
34. Leone L, Colato C, Girolomoni G. Prurigo pigmentosa in a pregnant woman. Int J Gynaecol Obstet 2007 Sep;98(3):261-2. [PubMed]
35. Wozel G, Blasum C, Winter C, Gerlach B. Dapsone hydroxylamine inhibits the LTB4-induced chemotaxis of polymorphonuclear leukocytes into human skin: Results of a pilot study. Inflamm Res 1997 Oct;46(10):420-2. [PubMed]
36. Degavre B, Guilhou JJ, Guillot B. Prurigo pigmentosa. Ann Dermatol Venereol 1994;121(1):46-9. [PubMed]
37. Stendahl O, Molin L, Dahlgren C. The inhibition of polymorphonuclear leukocyte cytotoxicity by dapsone. A possible mechanism in the treatment of dermatitis herpetiformis. J Clin Invest 1978 Jul;62(1):214-20. [PubMed]
38. Miyachi Y, Yoshioka A, Horio T, Imamura S, Niwa Y. Prurigo pigmentosa: A possible mechanism of action of sulfonamides. Dermatologica 1986;172(2):82-8. [PubMed]
39. Sugita K, Nishimura T. Effect of antimicrobial agents on chemotaxis of polymorphonuclear leukocytes. J Chemother 1995 Apr;7(2):118-25. [PubMed]
40. Ueyama Y, Misaki M, Ishihara Y, Matsumura T. Effects of antibiotics on human polymorphonuclear leukocyte chemotaxis in vitro. Br J Oral Maxillofac Surg 1994 Apr;32(2):96-9. [PubMed]
41. Schepis C, Siragusa M, Palazzo R, Ussia AF, Cavallari V. Prurigo pigmentosa treated with minocycline. Br J Dermatol 1996 Jul;135(1):158-9. [PubMed]
42. Siragusa M, Schepis C, Palazzo R, Fabrizi G, Guarneri B, Del Gracco S, Spada RS, Ferri R. Skin pathology findings in a cohort of 1500 adult and elderly subjects. Int J Dermatol 1999 May;38(5):361-6. [PubMed]
43. Shannon JF, Weedon D, Sharkey MP. Prurigo pigmentosa. Australas J Dermatol 2006 Nov;47(4):289-90. [PubMed]
44. Asgari M, Daneshpazhooh M, Chams Davatchi C, Boer A. Prurigo pigmentosa: An underdiagnosed disease in patients of Iranian descent? J Am Acad Dermatol 2006 Jul;55(1):131-6. [PubMed]
45. Yanguas I, Goday JJ, Gonzalez-Guemes M, Berridi D, Lozano M, Soloeta R. Prurigo pigmentosa in a white woman. J Am Acad Dermatol 1996 Sep;35(3 Pt 1):473-5. [PubMed]
46. Gurses L, Gurbuz O, Demircay Z, Kotiloglu E. Prurigo pigmentosa. Int J Dermatol 1999 Dec;38(12):924-5. [PubMed]
47. Baykal C, Buyukbabani N, Akinturk S, Saglik E. Prurigo pigmentosa: Not an uncommon disease in the Turkish population. Int J Dermatol 2006 Oct;45(10):1164-8. [PubMed]
48. Ekmekci TR, Altunay IK, Koslu A. Prurigo pigmentosa treated with doxycycline. Dermatol Online J 2006 Jan 27;12(1):9. [PubMed]
49. Schepis C, Siragusa M, Palazzo R, Cavallari V. Prurigo pigmentosa: A misdiagnosed dermatitis in Sicily. Cutis 1999 Feb;63(2):99-102. [PubMed]
50. Chiam LYT, Goh BK, Lim S, Ng SK. Prurigo pigmentosa: a report of two cases that responded to minocycline. Clin Exp Dermatol 2008;34:584-586. [PubMed]
51. Rodriguez-Diaz E, Blanco S, Alvarez-Cuesta C, Galache C, Barrio A, Corte G. Prurigo pigmentosa. Actas Dermosifiliogr 2005 Sep;96(7):441-5. [PubMed]
52. Yazawa N, Ihn H, Yamane K, Etoh T, Tamaki K. The successful treatment of prurigo pigmentosa with macrolide antibiotics. Dermatology 2001;202(1):67-9. [PubMed]
53. Akoglu G, Boztepe G, Karaduman A. Prurigo pigmentosa successfully treated with low-dose isotretinoin. Dermatology 2006;213(4):331-3. [PubMed]
© 2011 Dermatology Online Journal