Five—
The Image of the Hysteric
Sander L. Gilman
The Function of the "Real" Image of the Hysteric in Defining the Nature of Hysteria
In the history of hysteria one image haunts the eye. It is an 1887 painting by André Brouillet of Jean-Martin Charcot presenting his pet hysteric, "Blanche" (Blanche Wittman), to the members of his neurological service at the Salpêtrière.[1] This portrait, clearly standing within the great tradition of Rembrandt's anatomies and echoing the 1876 portrait, Pinel Freeing the Insane , by Tony Robert-Fleury, which hung in the main lecture hall at the Salpêtrière, has one rather anomalous moment. (Brouillet [1824-1908] was after all a student of Gérôme, whose history paintings always hide a mystery.) All of Charcot's staff are men, with the exception of the one nurse, who is about to catch the somnambulistic patient. Only these two women are placed in such a manner so as to see the rear of the hall; all of the male figures have their backs (or sides) to the rear. And on the rear wall is an enlarged drawing by Charcot's colleague Paul Richer of the arc-en-cercle stage of "grand" hysteria. Charcot described this stage in an 1877 lecture: "The patient suddenly falls to the ground, with a shrill cry; loss of consciousness is complete. The tetanic rigidity of all her members, which generally inaugurates the scene, is carried to a high degree; the body is forcibly bent backwards, the abdomen is prominent, greatly distended, and very resisting."[2] In Broulliet's engraving, Richer literally sits at Charcot's right hand, sketching the patient who is replicating his own drawing.[3] Only the women see (and "know," that is, act upon) the image of the hysteric. Their image of the hysteric, both as patient and as health-care practitioner is con-
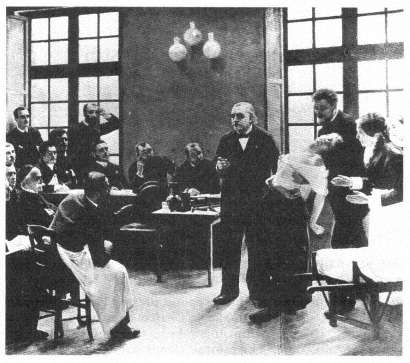
André Brouillet's image of Jean-Martin Charcot presenting his "pet" hysteric,
"Blanche" (Blanche Wittman), to the members of his neurological service at
the Salpêtrière (1887).
(Bethesda, Md.: National Library of Medicine.)
sciously formed by the visual image of the hysteric as created by a male physician.
The late nineteenth century understood such a pattern as the very model for knowing the world. Oscar Wilde suggested that we learn about nature from the work of art. "External nature," according to Wilde, "imitates Art. The only effects that she can show us are effects that we have already seen through poetry, or in paintings."[4] And, we might add, in photographs.[5] This is precisely what Blanche Wittman did at the Salpêtrière, as she learned from the representations of the hysteric how to appear as a hysteric.[6]
This image does not stand alone but is representative of a series of representations of the hysteric during the latter half of the nineteenth century. In the Jacques-Joseph Moreau de Tours 1890 image, Hysterics of the Charité on the Service of Dr. Luys , a wider range of representa-
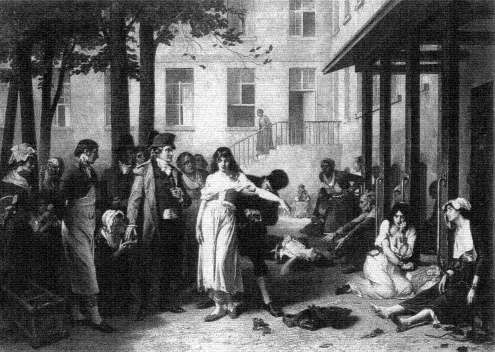
Tony Robert-Fleury's Pinel Freeing the Insane (1876), which hung in the
main lecture hall at the Salpêtrière.
(Paris: The Library of the Salpêtrière.)

Jacques-Joseph Moreau de Tours, Hysterics of the Charité on the Service of Dr. Luys (1890).
(Bethesda, Md.: National Library of Medicine.)
Photo courtesy Yale Medical Library.
tions of the hysteric is present.[7] Dr. J.-B. Luys (1848-1897), the author of an early photographic medical atlas,[8] stands to the rear of the room, with his white mutton-chop whiskers, as his female patients perform. (Moreau de Tour had himself been an intern under J.-É.-D. Esquirol, the creator of the first modern psychiatric atlas, at Charenton.[9] ) Luys had described and photographed the hysterics of the Salpêtrière for his 1887 study of the effects of hypnotism as therapy.[10] All of the patients in Moreau de Tours's image are seemingly oblivious to what immediately captures the eye of the viewer. On the rear wall of this ward, a permanent fixture of the room inhabited by the patients, is a chart recording the different phases of hypnosis, the stages that the patient is expected to pass through as she performs for her male audience. It is part of the world of the patient, a means through which to learn how to structure one's hysteria so as to make one an exemplary patient. Indeed, this is paralleled within the images that are so central to Jules Luys's own work, by the photographs of his pet patients, especially "Esther," taken by his brother Georges, which illustrate his-1887 study of the emotions of the hysteric.[11]
These patients are seen. There is no attempt to mask their identity. In the case studies of the period (even as early as Pinel) there is the use of initials or masked names. But in the visual images that Esquirol brings there is the assumption that the face (its structure or its expression) is so important that it does not need to be masked. But there is also the understanding, given the artistic license of the engraving and the lithograph, that there would be sufficient difference between the image of the patient and the final representation as to mask the patient's identity. (This is not always the case, as one can see in Georges-François-Marie Gabriel's admittedly unpublished image of Eugéne Hugo, the brother of the author.[12] ) The exception to this seems to prove the rule. In the Nouvelle iconographie de la Salpêtrière , Charcot's house organ, there are rarely images of patients that are intentionally masked, usually naked women, such as the image of a young anorexic female reproduced in the fifth volume.[13] (The Nouvelle iconographie de la Salpêtrière is not the only journal of its type. The Revue photographique des Hôpitaux des Paris flourished in the 1870s.)
The importance of the image of the hysteric represented as learning from the medical images that surround her can be gleaned from the following anecdote. In an account of Charcot's experiments with hypnotism in the British Medical Journal of 5 October 1878, Arthur Gamgee, Professor of Physiology at Owens College, Manchester, observed:
One of the patients was suspected of stealing some photographs from the hospital, but she indignantly denied the charge. One morning [Mr.]
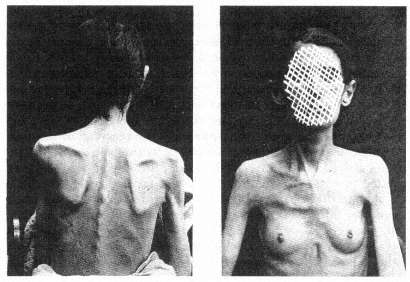
The masked image of the hysteric. From Louis Battaille, "Deux Cas
d'Anorexie Hystérique," Nouvelles Iconographie de la
Salpêtrière 5 (1892), plate opposite p. 277.
Photo courtesy Wellcome Institute Library, London.
Richer, after having made some experiments upon other subjects, found the suspected thief with her hand in the drawer containing the photographs, having already concealed some of them in her pocket. [Mr.] Richer approached her. She did not move; she was fixed—she was transformed into a statue, so to speak. The blows on the gong made in the adjoining ward had rendered her cataleptic at the very moment when, away from the observation of all, she committed the theft.[14]
It is Paul Richer, the creator of the archetypal image, the ornament of the lecture room in which rounds were held, who captures the "cataleptic" woman, a figure so mired in her internalization of his idea of the hysteric that she literally freezes as an incidental occurrence to the "experiment" taking place just beyond her ken.[15] This is not the world of Charcot in the role of Pinel "freeing the insane," whose image graced the public lecture hall in which the so-called Tuesday lectures took place. For here the "insane" patient is captured rather than freed by the intervention, no matter how incidental, by the physician. But why is this woman stealing photographs?[16] And whose photographs are they?
The photographs are those of the exemplary patient taken by Albert Londe, the head of the photographic service at the Salpêtrière, indeed

The hypnotized patient and the tuning fork. From Paul Richer, "Gonflement
du cou chez un hystérique," Nouvelles Iconographie de la Salpêtrière 2
(1889), plate 34.
Photo courtesy Wellcome Institute Library, London.
the first professional photographer to have a full-time appointment in any hospital in Europe. His job was to document the progress and manifestation of the patient's disease, to capture the stages and processes as they represented themselves on the visible surface of the patient, on the patient's physiognomy, posture, actions, as a means of cataloging the disease process. This Linnaean means of describing illnesses through their visible signs and symptoms (to use Jean-Martin Charcot's term, taken from the witch-hunting manuals of the Inquisition, the stigmata of the illness, from the stigmata diaboli that marked the body of the witch) dominated nineteenth-century European, but especially French, psychiatry. To describe was to understand, to describe in the most accurate manner meant to avoid the ambiguity of words, and to rely on the immediate, real image of the sufferer.
But the malleability of the symptoms in hysteria troubled the fin-de-siècle scientist. As Charcot noted, "Symptoms . . . have their destiny: Habent sua fata ." Symptoms, "after having enjoyed a certain degree of favour, doubtless on account of the theoretical considerations connected with [them, have] gone somewhat out of fashion . . ." But this is to be understood from the standpoint only of the physician-nosologist; from the standpoint of the patient, the symptoms are real, even if the patients are duplicitous: "You will meet with [simulation] at every step in the history of hysteria, and one finds himself sometimes admiring the amazing craft, sagacity, and perseverance which women, under the influence of this great neurosis, will put in play for the purposes of deception—especially when the physician is to be the victim. . . . It is incontestable that, in a multitude of cases, they have taken pleasure in distorting, by exaggerations, the principal circumstances of their disorder, in order to make them appear extraordinary and wonderful."[17] This deception is, for Charcot and his time, an absolute sign of the hysteric, and it can only be read correctly by a good diagnostician.
For hysteria must be "seen" to have observable symptoms, such as the changes of the skin or the wasting of the body, to be understood as a real disease: "Hysteria is a real disease, as real as small-pox or cancer, and . . . it has a physical basis, probably of a chemical nature, although this is yet very imperfectly understood."[18] As an early review of the first major journal from the Salpêtrière devoted to the visual representation of the insane noted, the camera was as necessary for the study of hysteria as the microscope was for histology.[19] This fantasy of realism captured the belief of the nineteenth century, both the doctor's and the patient's. For the doctor, the image is the patient, as it is for the patient. This search for an ontological representation of illness parallels the undertak-
ing of the exemplary fin-de-siècle scientist, Louis Pasteur, whose germ theory of contagious disease relied on the visibility of the germ for its power.[20] As Georges Canguilhem notes: "After all, a germ can be seen, even if this requires the complicated mediation of a microscope, stains and cultures, while we would never be able to see a miasma or an influence."[21] To see the patient means to develop the technique for seeing, a technique that is "scientific"; the patient, in turn, as the object of the medical gaze becomes part of the process of the creation of an ontological representation of the disease, a representation that is labeled hysteria. This does not deny the underlying pathology of the hysteric; it reflects only the meaning attributed to the symptoms created to represent the pathology as a disease.
One can speculate on whether the official nosology of American (and increasingly, world) clinical psychiatry, the DSM-IIIR (soon to be DSM-IV), in its restructuring of hysterical neurosis into conversion disorder, dissociative disorder, histrionic personality disorder, and brief reactive psychosis, did more than relabel an existing disease or whether these new labels are the self-conscious description of the manifestation of the hysteric in the 1980s.[22] But at least the compilers of DSM-IIIR saw their undertaking as the description of the disease, rather than as the search for its etiology. This does not mean, however, that the physician and the patient place any less reliance on the meaning of these definitions in order to shape our contemporary sense of the patient. How many patients today learn to have "conversion disorders" or "factitious disorders with psychological symptoms" from the medicalized world in which they—the sufferers from the dis-ease of hysteria—must function?
For the patient knows how to be a patient, as we see mirrored so well in André Brouillet's image of Charcot, only from the representation of the way the physician wishes to see (and therefore to know) the patient as the vessel of a disease, not any disease, but the disease of images and imagining, hysteria. It is this shared sense of the importance of the image, for the doctor as well as for the patient, which is reflected in the image of the hysteric.
Toward a Theory of "Realistic Representation" in Nineteenth-Century Thought
In my work on Hugh W. Diamond's mid-nineteenth-century introduction of photography into the treatment of the mentally ill, I was struck by the fact that Diamond believed he could cure at least some of his patients by exposing them to photographs of themselves. The "realism"

Hugh W. Diamond, a portrait of a case of "religious
melancholy."
(London: Royal Society of Medicine.)
of the photograph was assumed to have a therapeutic function because of its mode of representation. Such a view underlined the importance of all images for the alienists of the nineteenth century. Thus there was a constant striving for verisimilitude, not only for nosological purposes (that is, in order to categorize the illness) but also for therapeutic reasons. Seeing one's own difference provided the "healthy" aspect of the mind with the juxtaposition between the "normal" and the "abnormal." The desire to see the absolute border between these states encouraged the nineteenth-century scientist to seek out and "see" the difference. As Friedrich Nietzsche put it (paraphrasing Claude Bernard): "It is the
value of all morbid states that they show us under a magnifying glass certain states that are normal—but not easily visible when normal."[23] Disease itself is seen as a means of "seeing" the normal. And normality is an unself-conscious state like that of observers, who are never aware of that role until they self-consciously begin to think of themselves as observers through their training as "scientists" and, therefore, become aware of the meaning attached to the act of seeing.
But it was only with the introduction of the photograph that the power of such contrast—for the patient—was clearly articulated. Diamond stated in his 1856 paper "On the Application of Photography to the Physiognomic and Mental Phenomena of Insanity," read before the Royal Society, that "there is another point of view in which the value of portraits of the insane is peculiarly marked—viz. in the effect which they produce upon the patients themselves—I have had many opportunities of witnessing this effect—In very many cases they are examined with much pleasure and interest, but more particularly in those which mark the progress and cure of a severe attack of Mental Aberration."[24]
Diamond's course of treatment was straightforward. He presented his patients with images of themselves that seemed to startle them into an awareness of their madness, because of the radically realistic image of them as demented. Through this confrontation with a "realistic" image of their insane physiognomy, they began to realize their own altered perception of reality. In his talk, he presented the case of "A. D., aged 20," whose "delusions consisted in the supposed possession of great wealth and of an exalted station as a queen."[25] He photographed her. Her reaction to the images she saw reflected the "startle" effect inherent in the newness of the medium of photography: "Her subsequent amusement in seeing the portraits [of herself in various stages of her illness] and her frequent conversation about them was the first decided step in her gradual improvement, and about four months ago she was discharged perfectly cured, and laughed heartily at her former imaginations."[26] If we can extend Diamond's argument, we can suppose that the nineteenth-century alienist saw the patient-observer as sharing the implication of the photographic image, the startle effect that accompanied the introduction of this new medium of representation.
In further work on the use of photography as a means of psychotherapy, I discovered that other alienists of the period, such as Sir William Charles Hood, the director of the Bethlem Asylum, undertook similar applications of photography. I initially extrapolated certain broader generalities about the reaction to the photograph by the first generation to see photographs after their invention in 1839. (This first period oc-
curred a full decade later in Great Britain than in the rest of Europe because both Daguerre's and Fox Talbot's methods of fixing images were under patent during the 1840s only in Great Britain. In the rest of Europe, the daguerreotype at least was in the public domain by the early 1840s.) I believed that the earliest photographs were such a radical mode of representing the reality of the self as different that they had some type of psychological shock effect. That is, they so disoriented patients as to where the already distorted line between what is real or unreal lay, that patients were forced to reexamine their own psychological confusions. I was convinced, however, that it was the perception of the self, the image of the self as the mad person, which caused the "startle" effect.[27] And that was the radical difference of the photograph, as perceived by those in this first generation to see photographs.
George S. Layne, in an essay in 1981, contradicted this finding, while still supporting my sense of the radical break with existing models of perception.[28] He uncovered the fact that the brothers William and Frederick Langenheim provided lantern slides for the "moral" treatment of the patients in the Philadelphia Hospital for the Insane a year before (1851) Diamond exposed his patients to their own images in the Surrey County Lunatic Asylum. But the Langenheim images were not of the patients, but rather were general images such as landscapes and street scenes, yet they had shock value in treating the patients. So it seemed to be not the image of the self but the radical newness of the medium that caused the "startle" effect.
One of the reasons that the "startle" effect was so pronounced as to be useful in therapy in the public asylums was that the working-class inmates of the asylums did not share the bourgeois and upper-class tradition of seeing and understanding visual objects which had developed out of the "realistic" philosophy of Enlightenment art. Even prints and engravings, understood as aesthetic objects, had been, for the most part, out of the financial reach of the proletariat. Theirs was a world with limited access to images—the absence of cheap illustrated newspapers (soon to appear in Great Britain in the middle-class form of the Graphic and the Illustrated London News ) meant that their world of images was the crude broadside with its lithographed (or indeed woodcut) image. But the middle and upper classes had a tradition of seeing and speaking about art, at least in terms of the reproduction of the work of art as engravings (such as the Broulliet and Moreau de Tours images). For them, even if the "startle" effect occurred (or perhaps because it occurred), the objects recorded were understood in terms of a historical continuity of perceiving aesthetic images. And, indeed, the entire history
of early photography is full of references to the continuity of the photograph with earlier modes of representation. A letter from Elizabeth Barrett Browning as late as 1843 reflects both the "startle" effect and the language in which it was articulated:
My dearest Miss Mitford, do you know anything about that wonderful invention of the day, called the Daguerreotype?—that is, have you seen any portraits produced by means of it? Think of a man sitting down in the sun and leaving his facsimile in all its full completion of outline and shadow, steadfast on a plate, at the end of a minute and a half! The Mesmeric disembodiment of spirits strikes one as a degree less marvellous. And several of these wonderful portraits . . . like engravings—only exquisite and delicate beyond the work of the engraver—have I seen lately—longing to have such a memorial of every Being dear to me in the world. It is not merely the likeness which is precious in such cases—but the association, and the sense of nearness involved in the thing . . . the fact of the very shadow of the person lying there fixed for ever! It is the very sanctification of portraits I think and it is not at all monstrous in me to say what my brothers cry out against so vehemently . . . that I would rather have such a memorial of one I dearly loved, than the noblest Artist's work ever produced.[29]
Such photographic images were perceived as a clear continuation of other, older means of the reproduction of images. Elizabeth Barrett Browning's vocabulary is initially taken from that of one of the fine arts, engraving. She is startled by the perceived realism of the image, but she places it within the Victorian model of progress in the reproduction of visual images. The photograph seems to her to be "exquisite and delicate beyond the work of the engraver." And yet her perception of this new medium is such that it draws on the science of the day, mesmerism, with its own "startle" effect, as its initial analogy. And, indeed, the "art" of engraving is the most highly mechanical of all the fine arts of the period. These associations, first between the various modes of creating and reproducing images, and then between the aesthetic and the scientific, dominate the discourse of the first generation to view photographs.
Alexander von Humboldt, in a letter dated 7 January 1839 to the Duchess Friederike von Anhalt-Dessau, stresses this admixture: "Objects that express themselves in inimitable fidelity, light fixed by the art of chemistry to leave enduring traces within a few minutes and to circumscribe clearly even the most delicate parts of contours—to see all of this magic (admittedly without color) . . . certainly speaks incontrovertibly for reason and the power of imagination."[30] The mix of the language of science and the language of art is clear here with Humboldt's
perception of the photograph as the product of a science rooted in the imagination, but producing aesthetic objects (which he sees as flawed in part because of their colorlessness). Edgar Allan Poe, in one of his 1840 essays on the daguerreotype, makes many of the same verbal associations.[31] Thus the articulation of the "startle" effect in the middle and upper classes points to a confusion in the vocabulary in which this effect was to be addressed: Is it a continuation of the older forms of representation (and therefore to be considered "art") or is it a new and different mode of representation (and therefore to be considered "science")? What all were agreed upon in that first generation was that the images were "real." It was that "realism," prefigured by the aesthetic theory of the Enlightenment, which framed the perception of the photograph and which provided the vocabulary in which the "startle" effect was articulated. The presence of the "startle" effect would seem to be a universal among those individuals exposed to the first photographs. It is no surprise that the first photographer-physicians, such as Hugh Diamond, who incorporated the "image" within their mode of treatment, were also constrained to see (and to know) the photograph in terms of its "startle" effect.
It is with the general understanding of the function of the photograph that the aesthetic tradition of representing the mentally ill begins to be submerged and there evolves a sense of collaboration—already implicit in the meaning given to the realism of the photograph by doctor and patient alike—about the educative function of images. But it is in the different function of images of the patient and images of the physician that the application of this problem in the history of seeing is to be found. For with the craze for the carte-de-visite, which began in the 1850s, all gentlemen and gentlewomen had to have their pictures taken. Indeed, as I have argued elsewhere, the very absence of photographs of those who understood themselves to be part of the world of society is an interpretable fact.[32] How very different for those whose images are taken from them, the mentally ill, the criminal, the maimed. For their images do not grace the storefronts of the photographers; their images become ersatz representations of the nosology that they represent. These "real" images, these images that startle, are images of the disease and not of the patient. And again it is the movement from the aesthetic to the real, from the artistic to the therapeutic, from the image of the patient to the definition of the patient's reality that lies at the center of this world of images. The image is the essence of the patient, it gives the patient form. The patient, or at least the presentation of the patient, quickly becomes the creation of the physician's sense of the cor-
rectness of the patient's disease. With the hysteric, the very nature of the illness provides for the patient a demand for the forming touch of the authority, for the control implicit in the worldview that generates "real" images. For hysteria is the classic disease of the imagination—not of the uterus—as Charcot (and then Freud[33] ) understood. But the shaping of the imagination through the "realism" of the photograph lies behind the pilferage described in Gamgee's account of the Salpêtrière incident. For can we imagine that the patient in the Salpêtrière is stealing back her identity, her sense of self, in removing the image of the hysteric from the grasp of the physicians?
Medical and Aesthetic Models for the Representation of the Hysteric
The image of the hysteric does not simply arise out of Jean-Martin Char-cot's personal interest in the visual representation of the hysteric at the Salpêtrière.[34] Charcot does not invent the act of "seeing" hysteria. His own interests in capturing the visual aspect of his patients combined with his own perception of his hysterical patients to record the image of his patients as early as his first years at the Salpêtrière, the 1860s. Charcot comes to his task of understanding his patient with a long personal need to see and represent the patient. But his view is not unique, it is part of a long-standing European tradition of representing the insane, into which the image of the hysteric must be fitted. Indeed, it is a tradition which is as much popular as it is scientific. For Moreau de Tours's image provides us with another context for the structuring of the hysteric—the world of the hypnotizable patient, the image of the mesmerizable female. For hysteria, from the eighteenth century, is a disease of the imagination, not a disease of the womb.
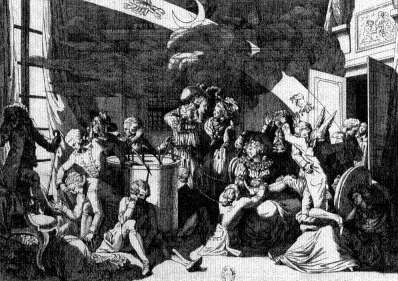
The image of the patients of the Viennese physician Franz Anton Mesmer and his students during the 1780s provides one of the keys to the representation of the hysteric at the end of the 1800s.[35] After his arrival in Paris in the winter of 1778, the representation of Mesmer becomes part of the tradition of representing the insane. In a contemporary cartoon reflecting a mesmerist session, it is not merely that the quack physician is indicated by his ass's ears. More important is that the patients gathered about the mesmerist's "tub" are represented in the traditional pose of the melancholic (with head on hand on knee) and the lovesick (swooning in the chair). The latter becomes identified retrospectively with the arc-en-cercle position of the hysteric (in some of the historical writing of the mid-twentieth century), because of the associa-
The image of the mesmerist.
(Paris: Bibliothèque nationale: Cabinet of Prints.)
tion of the hysteric with the sexual (in many different ways), while the melancholic vanishes from any consideration as a forerunner of the image of the hysteric. The visual representation of the mesmerist and the patient are all means of limiting the scope of the diseased to the identifiable individual.
The suppression of the political radicalism associated with one of the most influential groups under Nicolas Bergasse after the French Revolution meant that there was a general tendency to see the mesmeric patient as an asocial being who only shammed illness out of a sense of social uselessness. Likewise, the mesmerist was understood, not as a force for change, but as a quack. The cartoons of the patient and the physician from the 1780s had already carried that message. In one such image a mesmeric healer, wearing an ass head, begins to mesmerize a young, female sufferer.[36] Her position echoes the association of disease and sex-
The "ass-mesmerists."
(Paris: Bibliothèque nationale: Cabinet of Prints.)
uality in the arc-en-cercle position of the grand hysteric, as she begins to lie back in her chair as her moral seduction begins. Mirrored in the background is the representation of the sexual exploitation of the female patient by the mesmerist, warned against in the secret appendix to the Report of the Royal Commission on Mesmerism. Here the physician is as hypersexual as the patient.
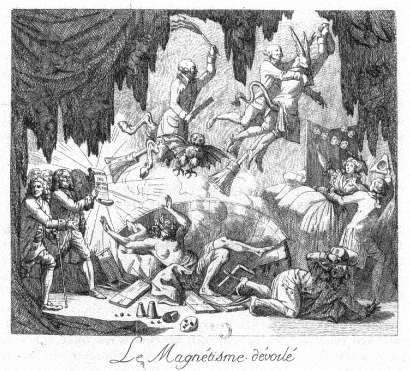
In another image the conceit of the ass-mesmerists is repeated.[37] They are being driven out of the scene by the shining truth of the report of the Royal Commission held by Benjamin Franklin. What is central to this image is that the mesmerists are represented as a compound sign. They are both madmen and devils. They are viewed as a parody of the images of the demonic evil spirits released from the mad as healed by Christ (and his saints) in the traditional iconography of madness. Here the split-hoofed image of the devil as well as the broomsticks associated with flying witches are employed. But this image of the healer is also that of the insane, for the split-hoofed figure is brandishing a scourge, which is one of the traditional icons of the insane. The figure of the arc-en-cercle in the representation of the patient is here reversed. The blindfolded, naked patient is seen in the closed mesmeric tub, not arched but collapsing inward. This can be seen as antithetical to another image of the mes-
merist healing process, the circle of "magnetized" hands, in which a seemingly unconscious female is represented in the left foreground; balancing the portrait of Mesmer, the healer, in the right foreground.[38] The imagery of this representation is tied to an understanding of the "meaning" of mesmerism and the mesmerist treatment in the course of the nineteenth century. The disrepute of the mesmerist, labeled as insane or demonically possessed, and thus in need of the sort of control represented by Franklin, Antoine-Laurent Lavoisier, and the Royal Commission, is carried over into the disrepute associated with the very naming of the treatment. The image of the physician, as well as the patient, is drawn into question in these associations. Such images remain associated with the idea of the hysteric through the visual representation of the patient.
The mesmerism patient is understood at the close of the nineteenth century to be one of the precursors of the fin-de-siècle hysteric. The image of the physician, as in the portraits of Charcot and Luys, must be quite different from that of the mesmerist; it must be separated from the image of the quack. Rather this image must be associated with the heroic image of the alienist, the image of Pinel as a force of social change (like Franklin). Merely changing the label of the mode of treatment from mesmerism to hypnotism or electrolization was not sufficient. The very relationship between the hysteric and the physician must be merged into the highest level of institutionalized medical representation—that of the image of science in the science of creating images.
The image of the hysteric in the medical literature of the nineteenth century is an essential image of deviance. It is an image that is taken—at least in its most radical form—out of another context. The central image of the hysteric, the essential attitudes passionnelles in Charcot's vocabulary of images, is a sign of quite a different disease—tetanus. The arc-en-cercle stage of Richer's image of grand hysteria (and its retrospective reading of the image of the swooning mesmerist patient) was consciously modeled on an image taken from the literature on the representation of anatomy and pathology for artists, rather than from a purely medical source.[39] Taken from the second edition of Sir Charles Bell's Essays on the Anatomy and Philosophy of Expression (1824), this image is rooted in a specific understanding of the nature of medical semiotics. Bell notes:
I throw in this sketch to remind the painter that in convulsion , although there may appear to him an accidental and deranged action of the muscular frame, there is no such thing in nature. It is a disease he is representing, which has definable symptoms, and it will ever present itself with the same characters.[40]
The range of the positions of the hysteric. Given best in Paul Richer, Études
cliniques sur le grande hystérie ou hystéro-épilepsie
(Paris: Delahaye & Lecrosnier, 1881), plate 5.
(Bethesda, Md.: National Library of Medicine.)

The opisthotonic position. From Sir Charles Bell's Essays on the
Anatomy and Philosophy of Expression (London: John Murray, 1824), p. 101.
(Bethesda, Md.: National Library of Medicine.)
Bell's observation may well hold true for tetanus, but the opisthotonic position chosen by him to represent the unalterability of the relationship between sign and causation is adapted by Charcot and later by Freud and given specific meaning in regard to the representation of the illness of the nerves and mind in the hysteric. One must note that Charcot is not the first "modern" scientist to call upon tetanus as his ontological representation for "seeing" the body. John Brown (1735-1788), in evolving the concept of the irritability of the muscles from the work of Albrecht von Hailer, argues that health and disease are not at all different states since the forces that produce each have the same action.[41] His example is a comparison of the normal contractions of the muscles and the pathological appearance of the opisthotonus in tetanus. The opisthotonus is one of the most striking manifestations of any disease. But it is also an almost infallible sign for the physician, since its outcome is almost surely negative. In a world in which the power of the physician lay, not in the ability to cure, but in the ability to foretell the course of a disease, the meaning of this sign for doctor and patient alike was clear. Thus Brown, Bell, and Charcot all call upon the image of the opisthotonus as a sign of the visual interpretability of disease and, therefore, the power of the physician's insight over the disease. At the end of the nineteenth century there was still a clear need to provide differential diagnosis between tetanus and hysteria for the practitioner. Among other signs, tetanus was described as presenting "persistent rigidity with
tendency to opisthotonos . . ." while hysteria presented "opisthotonos persistent, and intense rigidity between convulsions."[42] In seeing the patient, little distinction was made between organic and functional deficits.
Charcot in seeing the hysteric evolves his own system of representing the disease. He sees the hysteric as suffering from a weakness of the nerves and the disease as being caused by a trauma (such as an accident or violence). Thus the hysteric patient was predisposed to the disease—at least once he or she was exposed to some traumatic event. It is clear that Charcot evolved this view through his treatment of the patients at the Salpêtrière—epileptic and hysterical female patients who were as different from him (and his class) as was possible.[43] The counterargument to this view was evolved by John Hughlings Jackson, whose initial interest was sparked by his wife's epilepsy. This view was one of universal susceptibility. Seeing the disease as a pattern of the dissolution of the higher functions of the nervous system through the presence of a lesion, Jackson understands the symptoms of the hysteric as signs of the lower (and therefore earlier) functions of the nervous system. This evolutionary model sees the symptoms of the hysteric as signs of the structure of the more primitive psychic organization. Both views—the view that calls upon trauma and biological predeterminism as well as the view that calls upon the model of the nervous system being layered to represent the evolutionary history of the mind—come to be absorbed in the fin-de-siècle debates about hysteria.[44]
As early as 1888, Sigmund Freud calls up the figure of the opisthotonus in the context of attacks of hystero-epilepsy.[45] He continues this argument as late as 1908 when he understands coition to be a form of "minor epilepsy." For "a hysterical attack is the reflex mechanism of the act of coition—a mechanism which is ready to hand in everybody, including women, and which we see coming into manifest operation when an unrestrained surrender is made to sexual activity."[46] Thus Freud explains the opisthotonus as the antithesis of the embrace—the internalized enactment of coitus. But this is an image that does not vanish, but is rather consistently transmuted.
Freud uses the image of the opisthotonus as the antithetical image to coitus within his initial reworking of Charcot's nosological criteria. Seeing the reality of the opisthotonus as the key to the somatic nature of hysteria meant understanding the concept of trauma as existing in real experience rather than in fantasy. Sándor Ferenczi, in his clinical diary of 1932, can call upon "a case in which in relaxation ('trance') opisthotonic positions did appear: when contact could be established with the patient, she reported that the position was a reaction to a feeling of
painful excitation in the genital passage, which the patient described as painful hunger: in this position, psychic unpleasure and defense against ardent desire are simultaneously represented."[47] Ferenczi traces this reaction formation back to the actual seduction of the female child by her father. All of these references—and Charcot's own vocabulary of images, especially the opisthotonus—stem from a vocabulary of images which clearly (at least in the medical literature of the nineteenth century) defined the line between the healthy and the diseased. The opisthotonus is a sign of the presence of a disease—whether a form of hysteroepilepsy or a signifier of pathological sexuality or a real seduction.
There is a one-to-one relationship between the sign and the meaning. Given Freud's own complicated formulas for the generation of symbolic meaning, already documented in detail in his 1900 Interpretation of Dreams , it is striking that in returning to the subject matter of the hysteric, which he and Josef Breuer had begun to explain in 1895 as the result of the suppression of real traumatic events—that is, precisely the sort of seduction of children by adults in authority (parents) to which Ferenczi, quite opposed by Freud, returns some three decades later—he reverts to a pattern of explanation that relies on the meaning of the visual image.
The association between images of the tetanal opisthotonus is in no way limited to the neurological literature coming out of the Salpêtrière or out of the Viennese schools of psychoanalysis. During World War I, Arthur F. Hurst reflected on the relationship between the hysterical etiology of "war contractures" ("battle fatigue" or posttraumatic neurosis) as opposed to those contractures which have their origin in a localized infection.[48] For Hurst the question of the differential diagnosis of hysterical contracture (here localized in contrast to the full-body opisthotonus) as opposed to localized tetanus is questionable. It is clear that in time of war the duration of the cure—a "single sitting by persuasion and reeducation" in the first case or "months of treatment" in the latter—would place emphasis on seeing the majority of such cases as quickly healable. The assumption in Hurst's presentation is that the confusion between real (i.e., somatic) and hysterical contractures advocated by continental neurologists such as Josef Babinski and Jules Froment marks a faulty distinction between a biological and a psychological illness.[49] Such an argument would be parallel to Freud's attempt to collapse the distinction between real epilepsy and hysterical epilepsy. The images of the case of tetanus as opposed to the hysteric are, however, quite illuminating. For the half-body portrait of the soldier with his wound prominently displayed relates the image of the contracted arm
to the entire individual; the hysterical arm stands alone. Here the role of the representation of the arm comes to play a central role. The case described, that of "Sergt. M" who "was wounded in the right forearm on April 10, 1917," is "recognized as hysterical. . . as the deformity was identical with that shown in a photograph of a so-called reflex contracture in Babinski and Froment's book." It is the representation of the hysteric which defines the disease and which defines both the treatment of the disease and the patient's response: "On the day of admission the hand was continuously manipulated, the patient being persuaded at the same time that it would rapidly relax. In ten minutes complete relaxation was obtained and the deformity disappeared." The relationship between seeing correctly and the patient's response is here made absolute. As Elaine Showalter notes, the transition from the image of the female pet patient of nineteenth-century clinical psychiatry to the image of the male sufferer from traumatic neurosis (shell shock) meant a drastic realignment of the presuppositions of gender.[50] Hurst sees the male hysteric as ill but as quickly curable, a factor that sets the soldier apart from the long tradition of more or less professional (i.e., long-term) female patients at the Salpêtriére. What he teaches his hysterics is to see themselves as "men"—to confront their illness and return to service.
Jean-Martin Charcot (and his colleague Paul Richer) provide the reader (and viewer) of these late nineteenth-century images of the hysteric with a set of antecedent images from sources other than the unspoken one of the mesmerist.[51] In their study of the representation of the insane—specifically the hysteric in the art of the West—they create their own history and conclude it with a clinical chapter outlining their "universal" nosological categories of hysteria, which they see as "valid for all countries, all times, all races."[52] Charcot and Richer begin by outlining the representation of possession in religious art from the early middle ages through the seventeenth century. They offer sixty-seven illustrations, often in line form, to provide visual proof of the continuity between the images of the Catholic mystic and the modern hysteric. Beginning with the fifth-century representation of possession in the Romanesque mosaics of Ravenna to images of Saint Catherine of Sienna, Charcot and Richer begin to build their case for the parallel (and therefore the universality) of their visual categories of hysteria.
The assumption is that there is an explicit continuity between Catholic religious experience, as represented by the practitioners, and the neurological pathologies of nineteenth-century France.[53] Thus the aesthetic representation of ecstasy becomes a clinical sign of psychopathology. Their movement is however not merely on the level of the equation of

The image of the possessed as the hysteric. From J.-M. Charcot
and Paul Richer, Les Dénoniaques dans l'art (Paris: Adrien Delahaye
et Emile Lecrosnier, 1887), p. 4.
Photo courtesy Wellcome Institute Library, London.
the religious-aesthetic and the clinical. For they cite one image (and text) from the general realm of medicine, and that is Sir Charles Bell's image of opisthotonus. The passage they quote is identical to the one cited above. Their argument is that the image of opisthotonus is parallel to a number of the images of possession that they offer, specifically the early seventeenth-century image of Saint Nilus by Domenicho Zampieri called Domenichino (1581-1641). Like their discussion of a sketch for the child in Raphael's Transfiguration , there is a stated assumption that the reality of the symptoms of hysteria are exactly parallel to the immutable reality of the symptoms of tetanus. In their final chapter, on the contemporary representation of the hysteric, Charcot and Richer draw on the images of the stages of the "hysterical convulsion" which Charcot had established in the 1880s. The parodies of religious experiences, from the position of prayer to the position of crucifixion find their visual representations in this chapter,[54] as does the classic arc-en-cercle position of the opisthotonus taken from Bell.[55]
What is most striking from the viewpoint of the history of the representation of the hysteric is that there is a continuity to the overall reception of the image of the hysteric which transcends the school of the

One of the topoi used to depict the history of the hysteric is this sketch
for the child in Raphael's Transfiguration . From J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile
Lecrosnier, 1887), p. 29.
Photo courtesy Wellcome Institute Library, London.
The self-crucified hysteric. From J.-M. Charcot and Paul Richer, Les
Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier, 1887),
p. 100, lower image.
Photo courtesy Wellcome Institute Library, London.
Salpêtriére. Thus if we return to the British images taken from Arthur F. Hurst's study of hysterical contractures, we can see that Charcot and Richer, in citing images from Louis Basile Carré de Montgeron's account of the Jansenist miracles,[56] had already set the stage for the representation of the nonfunctional limb as a primary sign of hysteria. The link between the female and the victim of shell shock is made through the representation of the body part that makes them unable to be mobile in a society that demands mobility as a sign of group identity. The meaning ascribed to mobility from the eighteenth century to the twentieth century is quite different (the middle-class woman becomes a full member of the new religious sect when she is healed; the soldier returns to his fighting unit when he is healed). But central to the image of cure is the image of mobility. The visibly nonfunctional limb, with the alteration in gait or in posture, marks the hysteric as diseased. The images taken from the history of religion have already provided a model for the representation of the affected area as the target for healing. The analogy between the mentally ill and the enthusiastic and/or rigorous fundamentalism of religious schismatics such as the Jansenists had already been made by Philippe Pinel in the wake of the French Revolution. Citing a range of British sources in a French Catholic context, Pinel was forced to see the hypermoralism of the Jansenists as setting them apart from French society. He labeled them the pathological equivalents of the Methodists.[57] Charcot's citation of Jansenism as the central visual clue to the history of hysteria ties the image of the hysteric, not merely
The religious cure of the "hysteric." From Louis Basile Carré de Montgeron,
La verité des miracles operés par l'intercession de M. de Pêris et autres
appellans demontrée contre M. L'archevêque de Sens , 3 vols. (Cologne: Chez
les libraires de la Campagie, 1745-47), as reproduced in J.-M. Charcot and Paul
Richer, Les Démoniaques dans l'art (Paris: Adrien Delahaye et Emile Lecrosnier,
1887), p. 81.
Photo courtesy Wellcome Institute Library, London.
to "religion" but to the religion of spiritual excess, to religions such as Methodism and, in a specific manner that will be discussed below, to the mystical religion of the Eastern Jews.[58]
The religious rigidity and the enthusiasm of the Jansenists came to stand for the perversion of the spirit which was as pathological as the diseases of the hysteric. Paul Regnard brings a series of the attitudes passionnelles in his photographs of Augustine from the second volume of the Iconographie de la Salpêtriére .[59] These images mimic the positions of the Jansenists, but they are without doubt images of pathology. The parallels make both sets of images pathognomonic.[60] As with the images of the Jansenists, the images of the hysterics are closely associated with visual hallucinations, with the seeing of what is not there as a sign of the falsification of the imagination. William Hammond, in his 1876 history of hysteria, continued this "liberal" discourse of the Salpêtriére which associated disease and religion. He noted that "in these undeveloped forms of both diseases, as noticed among the Jansenist convulsionnaires, the affected individuals appeared as if struck by the sight of some object before unseen, and the contemplation of which filled them with the most ravishing joy."[61] Here the pathologization of seeing is the mirror image of the clinical gaze of Charcot, who sees the disease, the disease of the fantasy, the disease of religion.
Thus Charcot and Richer undertake what many scientists of the nineteenth and twentieth centuries do—to write the history of their own discovery in order to show its universality across time (if not across cultures). But this history of the representation of hysteria, drawing on the power of the new secularized religion of science in displacing its antecedent Christianity, becomes the model through which the hysteric is visually categorized. This tradition does not stop with Richer and Charcot. Students of Charcot's provide some of the later material. Henry Meige (after 1901 the editor of the Nouvelle Iconographie de la Salpêtriére ) and Jean Heitz both contribute essays to the Nouvelle Iconographie de la Salpêtriére on the artistic image of the hysteric well into the twentieth century.[62] Within the German tradition, the physician-historian-art critic Eugen Holländer incorporates many of these images in writing his history of the image of the impaired in classical art.[63] Holläinder quotes liberally from the same visual sources as Charcot and Richer—citing Raphael and the various images of religious possession. Jean Rousselot continues this image in his study of medicine in art into the post-World War II era.[64] His work begins with the representation of the Greeks, such as the Bacchic scene of "dying Bacchante," now in the Uffizi. He comments in his caption: "In point of fact, a depiction of hysteria. At

The representation of religious ecstasy as pathological sign. From
Paul Regnard, Les maladies épidémiques de l'esprit: sorcellerie magnétisme,
morphinisme, délire des grandeurs (Paris: E. Plon, Nourrit et Cie., 1887), p. 95.
The image is an engraving of a photograph taken from the Iconographie
de la Salpêtriée .
(Bethesda, Md.: National Library of Medicine.)
the far right, a hysterical woman, her body bent in the shape of an arc." All of these works assume a continuity of the meaning of the image of the hysteric from the ancient Greeks to their contemporaries. And all of them stress the continuity between the ancient representation of religious experience (rather than images of pathology) and modern experiences of disease (rather than religion). This asymmetry provides a powerful subtext for the association between images of religion and those labeled in the popular mind as being associated with categories constructed as or labeled as religious ones—such as the Catholic (or at least the Catholic cleric) and, in an equally complex manner, the Jew.
The "warfare between theology and science," to paraphrase the title of A. D. White's classic nineteenth-century study,[65] which is played out within the secularized Christian discourse of late nineteenth-century psychopathology, is nowhere more clearly evident than in Paul Regnard's 1887 monograph (with 120 images) on the visual relationship between magnetism, morphinism, and madness, which begins with the visual equation between the witch and the mad.[66] Regnard, a physician and the professor of physiology at the National School of Agronomy, was the coeditor (with Désire-Magloire Bourneville of the Bicêtre) of the original, three-volume edition of the Iconographie photographique de la Salpêtriére[67] as well as a well-received medical atlas.[68] His study of 1887, which is dedicated to "cher maitre," Charcot, assumes the interrelationship of all forms of mass hysteria. His first example is the witch. He provides a series of plates from Abraham Palingh's study of witchcraft to document the visual representation of the witch as the "grand hysteric."[69] In this context Regnard brings in other images of demonic possession from the Renaissance to the seventeenth century (p. 41), including—as one of the images that becomes standard to the repertoire of visual proof—the figure of the boy from Raphael's Transfiguration (P. 59).
It is assumed that these pathological positions are indicative of the association with other forms of possession, such as hysteria. To make this absolutely clear in the reader's eye, he reproduces, in the form of drawings which thus resemble the format of the earlier images he has reproduced, a series of photographic images from the Iconographie photographique de la Salpêtriére . Of these the image of the gaze, the hallucination as experienced by the observer rather than the hysteric, stands as the icon of pathology (p. 87). Regnard makes similar visual claims in associating the image of the hysteric with that of the sleepwalker, the drug addict, and the person suffering from monomania. Images are produced that draw on the visual association of abnormal states—there is
The image of the witch. From Abraham Palingh, 't Afgeruckt Mom-Aansight
der Tooverye: Daar in het bedrogh der gewaande Toverye, naakt ontdeckt,
en emt gezone Redenen en exemplen dezer Eeuwe aangewezen wort (Amsterdam:
Andries van Damme, 1725), p. 50, as used in Paul Regnard, Les maladies êpidémiques
de l'esprit: sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 19.
(Bethesda, Md.: National Library of Medicine.)
The representation of a visual hallucination, the centrality of the eye
and the gaze. From Paul Regnard, Les maladies êpidémiques de l'esprit:
sorcellerie magnétisme, morphinisme, délire des grandeurs (Paris: E. Plon,
Nourrit et Cie., 1887), p. 87.
(Bethesda, Md.: National Library of Medicine.)
always the assumption that there is a normal image of the productive, healthy human, and the deviant is marked by external signs, such as position, clothing, handwriting, and so on. These signs represent the symptoms of mental disorder, and all are interrelated because the signs are interrelated. But more than this is shown by moving from the witch (and the torture and cruelty inflicted on the witch [p. 33] to the miracles associated [as in Charcot] with healing the hysteric, to use his term [pp. 133, 135]. Religion and its hypocrisy, its antithetical relationship to the act of modern medical healing, are cited, and the cures of the church are ascribed to the nature of the disease entity—to hysteria. The cure of the disease of hysteria is the mass hysteria of religion. The model for this is the antiquated one of homeopathic medicine—like curing like. It is clear that Regnard, like Charcot and Richer, is looking for a more modern approach to therapy—to electrization or to the newly relabeled science of hypnotism—for their cure, not to religion. For the church, representing the institutionalization of religion in contemporary society, is the root cause of the hysteria, not its cure.
The other central model cited by Charcot and Richer in their scientific work is the model of the epileptic.[70] Stemming from Charcot's initial observations on his patients in the Salpêtriére showing the symptoms of "hystero-epilepsy" (his own composite category, which Freud borrowed), the visual image of the difference of the hysteric stems to no little degree from the tradition of representing the epileptic.[71] The image of the epileptic is in many ways parallel to that of the hysteric. Thus the "simulation" of the hysteric is paralleled by the "contradictions and exaggerations of sentiment [which] are salient characteristics of epileptics," according to Cesare Lombroso. He continues: "Epilepsy has a disastrous effect on the character. It destroys the moral sense, causes irritability, alters the sensations through constant hallucinations and delusions, deadens the natural feelings or leads them into morbid channels."[72] This need to see the pathological character of the epileptic as parallel to his or her disease is replicated in the visual image of the epileptic. While many of the visual images of the epileptic in the medical literature of the nineteenth century deal with the problems of localizing the brain lesion,[73] there is also a tradition of representing the symptoms of epilepsy through representing the patient. Charles Féré, in the Nouvelle Iconographie de la Salpêtriére , represents hysteria as literally written on the skin of the hysteric.[74] The parallel image is to be found in the representation of hysterical ulceration.[75] If one examines L. Pierce Clark's argument from 1898 that there are "tetanoid seizures in epilepsy," one can see the argument coming full circle to the organic model

The sensitive skin of the epileptic becomes a tabula rasa upon which
the disease can be inscribed. From Charles Féré, "Note sur un cas de
mélanodermie récurrente chez un épileptique apathique," Nouvelle
iconographie de la Salpêtriére , 10 N.F. (1897): 332-339.
(Bethesda, Md.: National Library of Medicine.)
of tetanus.[76] Indeed, the fascination with the marking of the signs and symptoms of disease on the body permeates the image of the epileptic in ways other than the search for the Jacksonian brain "lesion" that must necessarily cause the seizures.[77] Thus there are images of the malformed hands of an epileptic woman or of the corporeal asymmetry of the epileptic female.[78]
The image of the epileptic is also found within the tradition of representing the physiognomy of the insane. Thus William Alexander provides the reader with a photograph of each of the patients whose cases he reports in his 1889 study in order to present their physiognomy.[79] It is the visual appearance of the epileptic that provides the clue to his or her special, hidden flaw. The lesion must, in some overt way, write itself on the body. Some essays, such as on the baldness[80] or the altered appearance of the hair[81] of an epileptic man as a sign of his illness, are more than reminiscent of the extraordinary images of the "plinca polonica" or "Judenkratze," the fantasy skin disease attributed by Western dermatologists to the Jews of the East. In some of the recent historical literature on the history of epilepsy, much of the same tradition cited by Charcot and Richer reappear—now in the context of documenting the ongoing history of epilepsy. Thus images of religious ecstasy and possession from the early Middle Ages appear as precursors of the image of the epileptic.[82]
All of these images relate to the idea of the hysteric as continuous over time and across cultures. This is the basic assumption of the definition of a positivistic disease entity at the close of the nineteenth century. Disease is real only if it is universal. And it is universal only if it can be seen and the act of seeing reproduced. This latter axiom is rarely stated (except by the head of the Salpêtriére's photographic service, Albert Londe), but it is assumed. Thus the image of the impaired patient is the touchstone for the reality of the disease.
Creating a Composite Image of the Hysteric
It is vital to understand that the creation of a history of the image of the hysteric is not the same thing as Charcot and Richer's attempt to place the diagnostic criteria applied to hysteria in the distant past (while ignoring the more recent past). What can be undertaken in a limited way (because of the extraordinary range of visual sources) is to sketch the visual aspects associated with the idea of hysteria at the turn of the century as a means of delineating the scope of the image. Thus this section will be devoted to a catalog of those visual qualities ascribed to the hys-
On the image of asymmetry of the epileptic, see plate XLI: "Asymetrie du
corps chez une epileptique," in F. Raymond and Pierre Janet, "Malformations
des mains en 'pinces de humard,'" Nouvelle iconographie de la Salpêtriée 10
(1897 ): 369-373 (an extract from their book Nécroses et idées fixes [Paris: F.
Alcan, 1898]).
Photo courtesy Wellcome Institute Library, London.
teric. We shall seek to sketch the boundaries of the representation of the visual nature of the hysteric in fin-de-siécle medical literature.
It is central to any understanding of this composite image that the desire of all of these studies, no matter what their national context, is to place themselves within the myth of the realism of the act of represen-

The face of the epileptic. From William Alexander, The Treatment of
Epilepsy (Edinburgh and London: Young J. Pentland, 1889), p. 107.
Photo courtesy Wellcome Institute Library, London.
tation and the highly specialized role that the physician (as interpreter) plays in reproducing and "reading" the image of the patient. And this reading has a clear relationship with the means of reproducing and disseminating the image of the hysteric. The startle effect has now blended into an idea of a realism that indicates a control by the scientist and the scientist alone over the new medium. (As anyone could make and possess photographs after the mid-1890s, it became more and more important for the scientific photograph to be the object of scientific interpretation. This attitude permitted many interpreters of the photograph of the patient seamlessly to become the interpreters of the new hermeticism of the X ray when it was introduced in 1895.) The reading of the photograph had also blended in with the aesthetic (or, perhaps better, artistic) tradition into which the "new" science of representation had placed the image of the hysteric. Charcot and Richer, in a paper they first published in the Journal of Nervous and Mental Disease in 1883, stated the case best. In noting the "immobile" physiognomy of a hysterical patient whose facial muscles had been electrically stimulated, they
Images of the alteration of the hair in the mentally ill are already evoked
in Darwin's study of the nature of expression. Here the image of the altered
appearance of the hair evokes older images of the diseases of the Eastern Jews.
From Dr. Räiuber, "Ein Fall von periodisch wiederkehrender Haarveräinderung
bei einem Epileptiker," [Virchows] Archiv für pathologische Anatomie und
Physiologie 97 (1884): 50-83, plate no. 2.
(Bethesda, Md.: National Library of Medicine.)
observe: "The physiognomy retained immobile, in a state of catalepsy. The same is true of the attitude and the gesture that accompanied it. The subject of this transformed into a sort of expressive statue, a motionless model, representing with striking accuracy most varied expressions, which artists, without doubt, might avail themselves of to a very great extent. The immobility of the attitudes thus provoked is eminently favorable to photographic reproduction."[83] They then reproduce a series of these photographs. This argument is similar to that critique by Walter Benjamin in his essay from the mid-1920s on the reproducibility of images in the age of technology.[84] For it is important to understand that observing is not sufficient. Charcot (and Richer) turn the object observed (the hysteric) into the work of art and then are able to commodify this work of art through the reproduction of her image within the scientific text. This is not quite like the cinematic examples that Benjamin brings. It is much more similar to the extensive photographic reproductions of "great works of art" which dominated the middle-class market for art during the 1880s and 1890s. Benjamin's discussion of the "exchange of glances" between the observed and the observer creates a critical context for the learning experience of the hysteric. For it seems that the exchange of glances in this system of representation is one between an aware hysteric and an unaware physician. But the Salpêtriére gave birth to other means of seeing difference and also of recording it.
In many of these images the confusion between acquired pathognomonic signs and inherent ones is manifest. There evolves in the finde-siécle discussion of the physiognomy the assumption that there is an absolute relationship between the form of the skull and the shape of the face.[85] And given the emphasis on craniometric measurements as a means of speaking about the nature of the mind/psyche it is clear that the relationship between the structure of the face and the mind, already present in the physiognomy of Johann Caspar Lavater (and his predecessors) becomes an easy one. Francis Warner summarizes many of the discussions of his contemporaries, such as Charles Darwin, in The Expression of Emotions in Men and Animals (1872).[86] Warner stresses the "results of cerebral action upon muscles" rather than the "shape of the brain case" in seeking to find the source for the asymmetry on the face of the hysteric. She describes, however, the existence of faces that "express intellectuality" and others that express "vulgarity." The latter are an example of the "coincident defective or coarse development of the brain-case and face." The former are the result of "the nerve-muscular condition of the face" and are "more directly indicative of the intellectuality of the brain; hence we should study a face as the index of the brain, when it
is seen in action as well as when at rest." This view can be seen as representative of the medical literature of physiognomy at the turn of the century. The stress on the asymmetry of the face, an asymmetry caused by the forces of the mind, rather than the marked "vulgarity" of the mental defective, can be traced back to Philippe Pinel and his representation of the "manic" and the "idiot" at the very beginning of the century. The concept of asymmetry (indeed all faces become asymmetrical with the passage of time) can introduce the importance of an aesthetics of the face of the hysteric.
James Shaw stresses the "swelling of the upper lip" in cases of "chronic hysterical insanity" as well as a "facial expression [that] often indicates the presence of migraine."[87] The face of the hysteric, specifically the hemiplegia that marks the face of the hysteric at the Salpêtriére, is an overt sign of difference. It is a distortion of the normal face—the baseline for the "beauty" of the individual.[88] Anthropological literature of the eighteenth and nineteenth centuries had debated the meaning of the varieties of beauty, especially female beauty, throughout the world.[89] The consensus was that there was a "great chain of beauty" running from the beautiful down to the ugly races which was paralleled within each race by a normative—that is, healthy—appearance as opposed to a sick appearance. This pathology of appearance underlies the representation of the asymmetrical, unaesthetic face of the hysteric. In a paper by Hurst (1918) on battle fatigue, the face of the hysteric marks the individual who can be quickly cured and sent back into battle.[90]
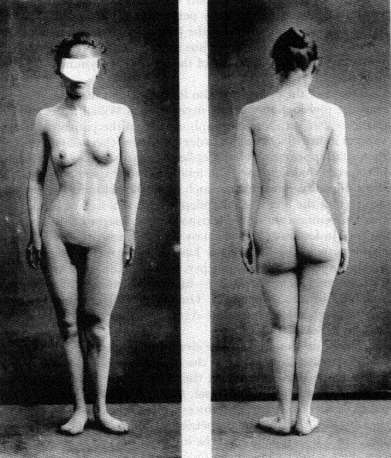
But if the face is marked, it is the eyes that provide the real clue. The stigmata that mark the face are most apparent in the representation of the eyes. For both the "look" of the hysteric and the gaze of the physician mark the hysteric. Building upon the nosology of hysterical blindness developed by Charcot as well as the Philadelphia ophthalmologist George Edmund de Schweinitz, Walter Baer Weidler traces the qualities of the eyes from the "contractures, spasms and palsies" of the "eyelids and extra-ocular muscles" (i.e., the representation of the appearance of the eye) to the manifestation of hysterical blindness (amblyopia or amaurosis, partial or complete loss of vision).[91] In the work of L. Lattes and A. Sacerdote from the 1920s, similar changes in the quality of the face are described in the case of a hysterical pseudo-hemorrhage of the eye.[92] It is the quality of the gaze in the photographs of the patients that is striking. The physical anomalies represented also provide the signs for the meaning read into the physiognomy. The drooping lids or the black eye add a quality of the abnormal, of the pathological, to the gaze of the patient, marking him or her as diseased.
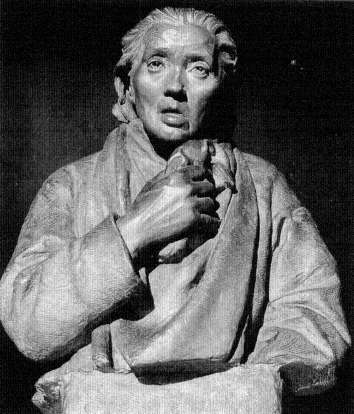
A sculpture of a case of hemiplegia from the teaching
collection of the Salpêtriére.
(Paris: The Salpêtriére.)
The disease that is sought is not in the eye. It is in the central nervous system, in the neural network that controls the eye. It is in the brain, the source of all hysteria, that the source of hysteria is to be found. The image of the brain becomes the image of the internal error of the hysteric. Jules Luys, in a paper of 1881, stresses this in both his text and in the accompanying images of localization.[93] E. Siemerling and J. Grasset see "cerebral-spinal degeneracy" as the source of hysteria.[94] In the work of the Hamburg physician Paul Steffens the localization of the lesion is represented in the post-mortem image of the brain.[95] All of these searches evoke the specter of the brain mythology that dominated much of the localization studies at the end of the century. The search after
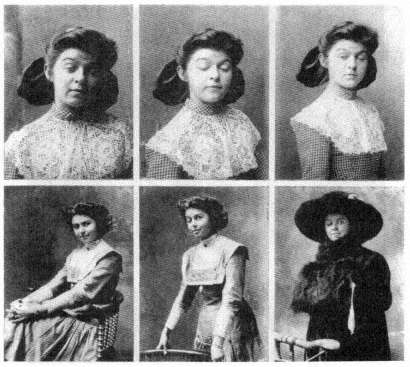
The eyes and the sight of the hysteric. From Walter Baer Weidler,
"Some Ocular Manifestations of Hysteria," International Clinics ,
22d ser. 2 (1912): 249-261. Plate (fig. 5) opposite p. 252.
Photo courtesy Wellcome Institute Library, London.
the source of the anomalous appearance of the hysteric was quite parallel to the search after the origins of other neurological disorders. A. Alzheimer represented such a search in his 1911 paper on cerebral plaques, using photographs of dyed brain specimens as his visual proof of their existence.[96]
All of these images were seen as having parallel value. Each of them demanded (according to their interpreter) a trained eye to see and represent the source of the error. The interrelationship between the scientific drawing and the photograph, both understood as veridical in localizing the source of the pathology, stressed the gaze of the scientist, in seeing the nature of the brain through the interpretation of the symptoms.
For the hysteric, the symptoms are often written on the body. The
The brain of the hysteric. From Jules Luys, "Recherches nouvelles
sur les hémiplégies émotives," L'Encephale: Journal des Maladies
Mentales et Nerveuses 1 (1881): 378-398, plate 7.
(Bethesda, Md.: National Library of Medicine.)
The brain structure of the hysteric. From C. von Höb lin and A.
Alzheimer, "Ein Beitrag zur Klinik und pathologischen Anatomie der
Westphal-Strümpellschen Pseudosklerose," Zeitschrift für die
gesamte Neurologie und Psychiatrie 8 (1911): 203.
Photo courtesy Wellcome Institute Library, London.
function of the skin as the map of the body is one of the oldest topoi of medicine. Reading the skin meant reading into the nature of the patient, his or her actions, and his or her resultant diseases. The nineteenth-century literature on masturbatory disease is full of such images,[97] as is, not surprisingly, the literature on hysteria. The ability of the hysterics to record written images on their skin, the hypersensitivity to touch, became one of the most fascinating symptoms for the fin-de-siécle physician. In the "modern" Revue de l'hypnotisme a striking image of such "skin writing" appears.[98] In Saint Petersburg the fin-de-siécle image of the hysteric was brought into the context of the stigmata, not Charcot's, but the stigmata of Christ.[99] The discussion of the patient presented in this "difficult case of hysteria" centered on the suggestibility of young Roman Catholic girls. The search after unique or strange manifestations
The ulcerated skin of the hysteric. From S. Weir Mitchell, "Hysterical
Rapid Respiration, With Cases; Peculiar Form of Rupial Skin Disease
in an Hysterical Woman," Transactions of the College of Physicians of
Philadelphia 14 (1892): 233.
(Bethesda, Md.: National Library of Medicine.)
of hysteria led S. Weir Mitchell, whose rest cure had been generally accepted as the treatment of choice by the end of the century, to examine a case of a hysterical ulcer in a twenty-four-year-old woman.[100] The differential diagnosis to this ulcer was to the ulceration of syphilis, which was "verified by the microscope." S. Róna continued the work that Moriz Kaposi had begun in Vienna, looking at specific forms of the manifestation of skin eruptions which could be labeled hysteric.[101] Thomas D. Savill, in London, undertook a similar study of the skin of his child patients and saw their hysteria inscribed thereupon.[102] In 1900 Dr. Bettmann from the Heidelberg Clinic of Wilhelm Erb described a further case of "atypical" skin inflammation in the hysteric; in 1901, a case of hysterical gangrene was described in Buffalo; in 1919, a similar case in Pisa. By 1930 a major survey of the nature of hysterical skin diseases was produced by Roberto Casazza in Pavia.[103] All of these studies (and more) are extensively illustrated. All of them relate, on one level or another, to the general assumption (countered by Jean-Martin Charcot in his theory of hysteria) that syphilis or the predisposition to syphilis played a major role in the risk for hysteria.
Many of these studies of the skin (such as that of Weir Mitchell) relate the appearance of the skin to the state of the genitalia, either in
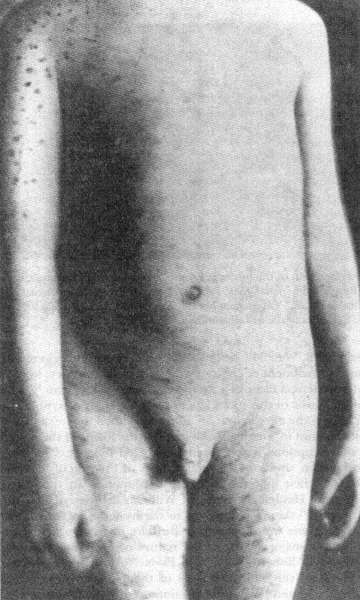
The association between the syphilitic and the hysteric was made as
much on dermatologic evidence (as seen on the skin) as on psychological
evidence. From Thomas D. Savill, "A Clinical Lecture on Hysterical Skin
Symptoms and Eruptions," The Lancet (January 30, 1904): 273-278, p. 276.
(Bethesda, Md.: National Library of Medicine.)
terms of gynecological examinations that are part of the case study or in terms of a discussion of the appearance of the skin in the genital regions. Charcot associated hysteria with the area of the ovaries, those areas of heightened sensitivity in the hysteric, a touch upon which could actually create hysterical episodes. This fascination with the compression of the ovaries as therapy as well as etiology is linked in the medical discourse of the period with the fascination about hysterical ischuria, the retention of urine and feces. The number of charts of the genital regions are legion, yet the number of detailed (and illustrated) studies of the form and structure of the genitalia are few. De Sinéty, a histologist at the College de France, published a series of unillustrated case studies of the genitalia of female hysterics in the mid-1870s, supporting Charcot's thesis of the centrality of sexual stimulation for the creation of the hysterical episode.[104] With the introduction of X-ray analysis there was even an attempt to represent the pelvic structure of the hysterical female, as a means of representing the disease.[105] The X ray was but a technical innovation. For the fantasies about internalized hysteria had existed prior to Charcot.[106] In 1847 Eliogoro Guitti had presented an illustrated study of the hysterical gut.[107]
The representation of the extremities, especially the hand and the foot, reflect not only the importance laid upon the hand and foot as signs of religious possession (stigmata, paralysis) but also the physical signs associated with epilepsy. Paul Sollier presents a case of contracture of the hand in a male hysteric in the fourth volume of the Nouvelle Iconographie de la Salpêtriére .[108] Some of the studies, such as those of Hurst, concentrate on the problem of hysterical contractures, such as Charcot's "glove anaesthesia" in the hysterical traumatic paralysis of the hand; others on the appearance of the hand, its coloration (usually blue, according to Gilles de la Tourette[109] ) and marked swelling.[110] The legs are similarly examined for the contractures of "hysterical paraplegia" (and their cure).[111] The images taken from Charcot's schematic representation of areas of anesthesia reappear over and over again to illustrate cases of the diminished ability to feel (and often to move) the limbs.[112]
The visual representation of posture and paralysis is used as a mode of visual proof of Charcot's nosological categories.[113] In an essay from the very first issue of the Nouvelle Iconographie de la Salpêtriére in 1888, by Georges Gilles de la Tourette, we are not only made to see the hemiplegic patient but also his gait, through a schematic representation.[114] In this case, described by Henri Lamarque and Emile Bitot, there is a comment on the plate that they had intended to use a photograph but an accident at the last moment ruined the plate and they were forced to
The X ray permitted the physician to see within the hysteric.
From Jose M. Jorge, "Coxalgia histérica," Revista de la Asociacion
Medica Argentina 32 (1920): 18-29, plate opposite p. 80.
(Bethesda, Md.: National Library of Medicine.)
use a photolithograph. The form of the representation becomes central to its message. For the photograph remains more real than any other mode of representing the hysteric. Thus in an essay by Byrom Bramwell—one of the leading Scottish specialists on nervous diseases such as hysteria and, one can add, one of the leading believers in a set pathognomonic representation of disease—the photograph remains the central proof for the differential diagnosis between "hysteria" and its contractures and other forms of organic disease.[115] But this photograph has been quite evidently cut to remove the presence of the physician or nurse whose hands remain supporting the patient. A similar undertaking can be seen in the photograph contracture represented in the essay by A. Steindler in Iowa City, except here the patient is given a staff on which to rest.[116]
The realism of the photograph concentrates the gaze of the physician-reader on the representation of the disease in the image of the patient. Peter Davidson follows this lead with his presentation of a case of hystero-catalepsy from Liverpool.[117] The number and range of Davidson's
The hysterical gut as an internal manifestation of the disease.
Eliogoro Guitti, "Osservazioni Cliniche," Giornale per Servire ai
Progressi della Patologia e della Terapeutica , 2d ser. 22 (1847): 229-258,
plate following p. 258.
(Bethesda, Md.: National Library of Medicine.)
cases (running from rheumatoid arthritis to hystero-catalepsy) would have enabled the author to illustrate any (or indeed all) of his cases. He chose to illustrate the case of hystero-catalepsy. As late as in 1930, in an essay by Prince P. Barker, at the Veterans' Hospital in Tuskegee, Alabama, the image of the hysteric black comes to represent the image of the hysteric whose limbs are frozen.[118] Using Charcot's categories ex-
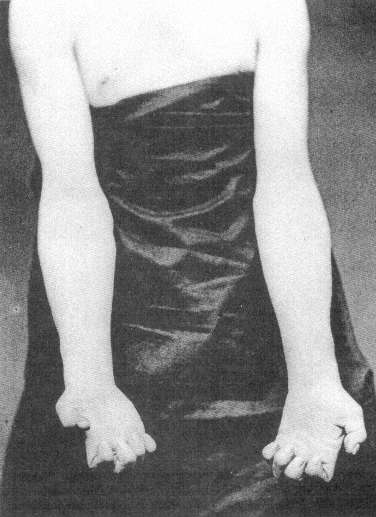
The hand of the male hysteric. From Paul Sollier, "Contracture Volontaire
chez un Hystérique," Nouvelles Iconographie de la Salpêtriére 4 (1891): 100-106,
plate opposite p. 106.
Photo courtesy Wellcome Institute Library, London.
The posture of the schematic "patient." From Henri Lamarque and
Emile Bitot, "Sur un cas d'hystérotraumatisrne chez l'homme,"
Bulletins de la Société d'Anatomie et de Physiologie Normales et
Pathologiques de Bordeaux 9 (1888): 242-257, plate with
figures 6 and 8.
(Bethesda, Md.: National Library of Medicine.)
A "doctored" photograph of the hysteric. From Byrom Bramwell, "Clinical
Lecture on a Case of Hysterical Contracture," Edinburgh Medical Journal ,
ns 1 (1897): 128-138, plate 5.
(Bethesda, Md.: National Library of Medicine.)
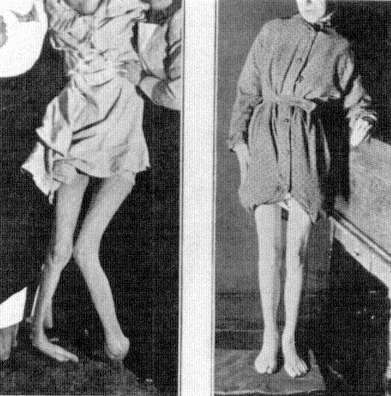
Above and verso: The hysteric posed. From A. Steindler, "On Hysterical
Contractures," International Clinics , 4th ser. 45 (1935): 221-229, fig. 2,
opposite p. 222.
Photos courtesy Wellcome Institute Library, London.
pressly, Barker shows three images. First, an image of the "normal," that is, pathological, posture of the patient; second, an image that in its blurred state is to represent the range of motion in the patient; and finally, an image of the body restored through "etherization and suggestion." Here the impact of the cinema on the idea of realism is evident. Whereas in the work of Lamarque and Bitot such an image would be understood as ruined, here it reveals a further aspect of the realism associated with the act of photographing.
One last form of realistic representation of the hysteric should be discussed. For throughout the vast literature of hysteria (and other forms of mental illness) in the nineteenth century there are uncountable
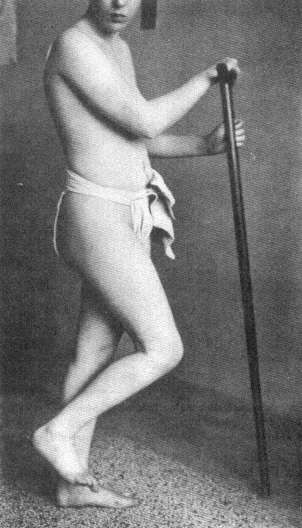
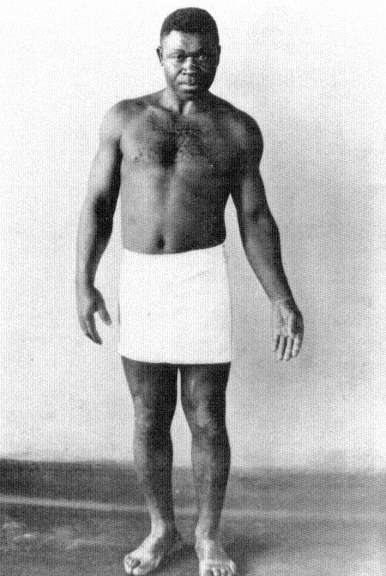
The illusion of movement in representing the hysteric. From Prince P.
Barker, "The Diagnosis and Treatment of Hysterical Paralysis," United
States Veteran's Bureau Medical Bulletin 6 (1930): 663-670, 3 plates
following p. 670.
(Bethesda, Md.: National Library of Medicine.)
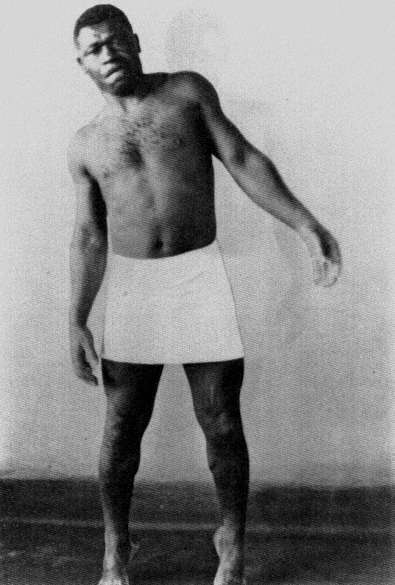
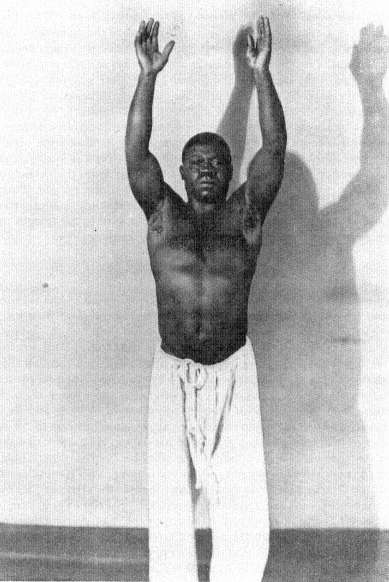
charts, graphs, and statistical tables. It is virtually unimportant what source one uses. From the medical periodicals in France[119] to those in Japan[120] or Germany,[121] one consistent image of the hysteric is that of the scientific reduction of the sufferer and the disease to schematic representations. The cry of these images is that they are the real, transcendent image of the hysteric. Like Galton's composite photographs (which will be discussed below), they give the observer an image of the totality of the disease. This fantasy of reducing the complexity of hysteria to statistics or charts rests on a notion of nineteenth-century science that everything is reducible to nonverbal form (read: mathematical), and that is precisely the claim of the photograph. For once, it is said, you eliminate narrative, you remove the subjective aspect from the evaluation of the disease and you have a real representation of the patient. Thus the use of charts and statistics in representing the hysteric is another visual means of creating an image of the disease, as sure as the images of the skin, or brain, or cellular structure of the hysteric.
Hysteria, Race, and Gender
Sigmund Freud's reading of the ancient Greek myth of the wandering womb, which, when lodged in the throat, created the globus hystericus , can serve us as a detailed example of the problems attendant to "seeing" the hysteric. It is well known that Freud, in the autobiographical account he wrote of the occasion some forty years after the event, recalled the bad reception that his initial paper on male hysteria had when he presented it before the Viennese Society of Physicians on 15 October 1886.[122] Returning from his work with Jean-Martin Charcot in Paris and desiring to present his newly acquired insights about male hysteria to his home audience in Vienna, Freud presented his paper. His powerful recollection was that his hearers thought that what he "said was incredible. . . . One of them, an old surgeon, actually broke out with the exclamation: 'But, my dear sir, how can you talk such nonsense? Hysteron [sic] means the uterus. So how can a man be hysterical?'"[123] Freud's angry memory was aimed at the narrow-minded claim of the Viennese establishment, that it, and it alone, had command of Greek. It was the young, French-trained Freud who knew that the concept of hysteria was tied to universals (which, at that point, he understood as trauma) and was not merely a reflex of the biological uniqueness of a subgroup. It was hysteria (the hallmark of the new science) that Freud wished to rescue from the crabbed claws of a Viennese medical establishment that could not even get its Greek correct, for hystera is the correct form of the Greek noun
The chart as the representation of the male hysteric in Japan, as in
the image of psychic forces in H. Nishi, "[Male Hysteria Cured by
Suggestion]," Chugai Iji Shinpo 405 (1897): 5-9; 406 (1897): 11-16,
image on p. 9.
(Bethesda, Md.: National Library of Medicine.)
The chart as the representation of the hysteric in Germany, as in the
evaluation of operations on the heating of the hysteric in K. Rudolphy,
"Ohroperationen bei Hysterischen," Zeitschrift für Ohrenheilkunde
und für die Krankheiten der Luftwege 44 (1903): 209-221, plate 17,
opposite p. 220.
(Bethesda, Md.: National Library of Medicine.)
for uterus. Thus the young Jew (and Freud understood himself from his exposure to the virulent "scientific" anti-Semitism of the Viennese University as a Jew) showed his command over not only the language of science (represented by Charcot's discourse on hysteria) but also the language of culture (Greek). (The significance of this factor will be shown in the course of this analysis.) Freud's understanding, like the understanding of his time, was that hysteria did not manifest itself as a disease of the womb but of the imagination. This did not absolve the female from being the group most at risk, however, for the idea of a pathological human imagination structurally replaced the image of the floating womb as the central etiology of hysteria. What was removed from the
category of hysteria as Freud brought it back to Vienna was its insistence on another group, the Jews, which replaced the woman as essentially at risk.
The idea of the hysteric was a central one for the imaginative world of Sigmund Freud as it was close to his self-definition. For at the close of the nineteenth century the idea of seeing the hysteric was closely bound to the idea of seeing the Jew—and very specifically the male Jew.[124] For if the visual representation of the hysteric within the world of images of the nineteenth century was the image of the female, its sub-text was that feminized males, such as Jews, were also hysterics, and they too could be "seen." The face of the Jew was as much a sign of the pathological as was the face of the hysteric. But even more so, the face of the Jew became the face of the hysteric. Let us quote from one of the defenders of the Jews against the charge of being tainted by hysteria. Maurice Fishberg's The Jews: A Study of Race and Environment (1911) states the case boldly: "The Jews, as is well known to every physician, are notorious sufferers of the functional disorders of the nervous system. Their nervous organization is constantly under strain, and the least injury will disturb its smooth workings."[125] The origin of this predisposition is neither consanguineous marriage ("the modern view . . . [is that they] are not at all detrimental to the health of the offspring") nor the occupations of the Jew ("hysteria [is] . . . met with in the poorer classes of Jews . . . as well as in the richer classes").[126] It is the result of the urban concentration of the Jews and "the repeated persecutions and abuses to which the Jews were subjected during the two thousand years of the Diaspora."[127] These influences, found at the turn of the century primarily among Eastern Jews, according to Fishberg show the predisposition of these specific groups of Jews to illnesses such as hysteria: "Organic as well as functional derangements of the nervous system are transmitted hereditarily from one generation to another."[128] It is not all Jews who are hysterics, but Eastern Jews, and primarily Eastern male Jews, according to Fishberg: "The Jewish population of [Warsaw] alone is almost exclusively the inexhaustible source for the supply of specimens of hysterical humanity, particularly the hysteria in the male, for all the clinics of Europe."[129] Here Fishberg, an American Jew, misquotes the French psychiatrist Fulgence Raymond, who had stated that Jews of Warsaw formed a major sector of the mentally ill of that city.[130] It was Fishberg's misquote of Raymond that became the standard view in German psychiatry.[131] It appeared within Freud's circle when Isidor Sadger noted at the 11 November 1908 meeting of the Vienna Psycho-
analytic Society: "In certain races (Russian and Polish Jews), almost every man is hysterical."[132] It is the male Jew from the East, from the provinces, who is most at risk for hysteria.
This view had been espoused by Charcot, who diagnosed on 19 February 1889 the case of a Hungarian Jew named Klein, "a true child of Ahasverus," as a case of male hysteria. Klein had a hysterical contracture of the hand and an extended numbness of the right arm and leg. It was Klein's limping that Charcot stressed. Klein "wandered sick and limping on foot to Paris" where he arrived on 11 December 1888. He appeared at the Salpêtrière the next day, "his feet so bloody that he could not leave his bed for many days." Klein "limped at the very beginning of his illness." Charcot reminded his listeners that the patient "is a Jew and that he has already revealed his pathological drives by his wanderings." His "travel-mania" could be seen in the fact that "as soon as he was on his feet again, he wanted to go to Brazil."[133] Klein also suffered from the standard numbness ascribed to the hysteric on half of his body. Wandering and limping mark the hysterical Jew as diseased, and diseased because of incestuous intermarriage.
H. Strauss of Berlin, in one of the most cited studies of the pathology of the Jews, provides a bar chart representing the risk of the Jews for hysteria.[134] It shows that male Jews suffer twice as often from hysteria as do male non-Jews. While it is clear that women still are the predominant sufferers from the disease, it shows a clear "feminization" of the male Jew in the context of the occurrence of hysteria. Freud's teacher, the liberal-Jewish neurologist Moriz Benedikt, also links the "American" quality of life with the appearance of hysteria, a disease that he understood as "a uniquely feminine nervous disease"—in men.[135] The struggle for life in the city causes the madness of the male Jew: "Mental anxiety and worry are the most frequent causes of mental breakdown. They are all excitable and live excitable lives, being constantly under the high pressure of business in town."[136] The reason for this inability to cope with the stresses of modern life lies in "hereditary influences," that is, their being Jews.[137]
And that is written on their faces, as on the faces of women. William Thackeray, in Codlingsby , his parody of Disraeli's novels, has his eponymous protagonist revel in the aestheticized sight of the "ringlets glossy, and curly, and jetty—eyes black as night—midsummer night—when it lightens; haughty noses bending like beaks of eagles—eager quivering nostrils—lips curved like the bow of Love" of the Jews.[138] "Every man or maiden," looks Jewish, but also looks feminine; "every babe or matron in that English Jewry bore in his countenance one or more of these
The Jewish hysteric, as represented by a chart from H. Strauss,
"Erkrankungen durch Alkohol und Syphilis bei den Juden," Zeitschrift
für Demographie und Statistik der Juden , 4 N.F. (1927): 33-39;
chart on p. 35.
(Bethesda, Md.: National Library of Medicine.)
The idealized "Jewish face," in a drawing by the famed fin-de-siècle
Viennese Jewish artist Ephraim Moses Lilien, is that of the female. In
Maurice Fishberg, The Jews: A Study of Race and Environment
(London: Walter Scott Publishing Co., 1911), p. 95.
Photo courtesy Wellcome Institute Library, London.
characteristics of his peerless Arab race." Codlingsby muses: "How beautiful they are!" when the jarring voice of Rafael Mendoza breaks his revery: "D'you vant to look at a nishe coat?" But the accent is not a true sign of the Jew's difference: "All traces of the accent with which he first addressed Lord Codlingsby had vanished, it was disguise: half the Hebrew's life is a disguise. He shields himself in craft, since the Norman boors persecuted him." The association between the falsity of the language of the Jews (which is not merely accented but duplicitous) is balanced by the "true" sight of the Jews—a factor that Thackeray parodies. What remains is that the "sight" of the Jew—the registration of the external signs of Jewishness—is a truer indicator of the nature of the Jew (or at least the perception of the Jew's nature in Thackeray's relativistic manner of representing the Jew) than is the mutable sign of the Jews' language, a language that is corrupted by as well as corrupting the world in which the Jew in the Diaspora lives.
Francis Galton actually tries to capture this "Jewish physiognomy" in his composite (i.e., multiple exposure) photographs of "boys in the Jews' Free School, Bell Lane." Galton provides types generated by multiple exposures. There he sees the "cold, scanning gaze" of the Jew as the sign of their difference, of their potential pathology.[139] It is in the Jews' gaze that the pathology can be found. This view is at least as old as Robert Burton's Anatomy of Melancholy , where Burton writes of the "goggle eyes" of the Jews, as well as "their voice, pace, gesture, [and] looks" as a sign of "their conditions and infirmities."[140] But it is not merely that Jews "look Jewish" but that this marks them as inferior: "Who has not heard people characterize such and such a man or woman they see in the streets as Jewish without in the least knowing anything about them? The street arab who calls out 'Jew' as some child hurries on to school is unconsciously giving the best and most disinterested proof that there is a reality in the Jewish expression."[141] The gaze of the non-Jew seeing the Jew is immediately translated into action.
The complexity of the Jewish response to this view can be measured in Joseph Jacob's discussion of Galton's finding of the absolute Jewish-ness of the gaze:
Cover up every part of composite A but the eyes, and yet I fancy any one familiar with Jews would say: "Those are Jewish eyes." I am less able to analyze this effect than in the case of the nose. . . . I fail to see any of the cold calculation which Mr. Galton noticed in the boys at the school, at any rate in the composites A, B, and C. There is something more like the dreamer and thinker than the merchant in A. In fact, on my showing this to an eminent painter of my acquaintance, he exclaimed, "I imagine that
Francis Galton's "composite" and "component" images of the Jew
(here the Jewish male stands as representative for the Jew). Frontispiece
to Joseph Jacobs, Studies in Jewish Statistics (London: D. Nutt, 1891).
Photo courtesy Wellcome Institute Library, London.
is how Spinoza looked when a lad," a piece of artistic insight which is remarkably confirmed by the portraits of the philosopher, though the artist had never seen one. The cold, somewhat hard look in composite D, however, is more confirmatory of Mr. Galton's impression. It is noteworthy that this is seen in a composite of young fellows between seventeen and twenty, who have had to fight a hard battle of life even by that early age.
For the Jewish social scientist such as Jacobs the inexplicable nature of the Jewish gaze exists (even more than the "nostrility" that characterizes the Jewish nose) to mark the Jew. His rationale is quite different than that of Galton—he seeks a social reason for the "hard and calculating" glance seen by Galton, but claims to see it nevertheless. This view reappears within the medical literature in the work of Jewish physicians, such as Moses Julius Gutmann, who writes of the structure of the Jewish face, of its typical form, as being the result of a combination of features that produce "the melancholy, pained expression" (the nebbish face) that is associated with the Jew. For Gutmann, and others, it is the result of the "psychological history of the Jew."[142]
Sigmund Freud's own fascination for Galton's "family" photographs must also be stressed. For Freud the composite photograph is virtually the representation of the dream in his Interpretation of Dreams (1990). It is an obsessive metaphor, which recurs throughout the course of his work.[143] The centrality of this metaphor is a residue of Freud's earlier acceptance of Charcot's reliance on the act of seeing as the privileged form of diagnosis. It is not seeing the unique but rather the universal. And yet hidden within those claims for universality are the images of race which Galton produces parallel to his other composites, in which the eyes of the Jew (read: Sigmund Freud) and his gaze are pathologized. The clinical gaze of the Jewish physician now becomes the object of the gaze of study. The image of the eyes, found in the calculating glance of the hysteric and the epileptic, reappears in the context of race.
In Henry Meige's dissertation of 1893 on the wandering Jew in the clinical setting of the Salpêtrière, the image of the Jew and the gaze of the Jew become one.[144] Meige undertakes to place the appearance of Eastern European (male) Jews in the Salpêtrière as a sign of the inherent instability of the Eastern European Jew. He sketches the background to the legend of the wandering Jew and provides (like his supervisor, Char-cot) a set of visual "images of Ahasverus." He then provides a series of case studies of Eastern (male) Jews, two of which he illustrates. The first plate is of "Moser C. called Moses," a forty-five- or forty-six-year-old Polish Jew from Warsaw who had already wandered through the clinics in Vienna and elsewhere; the second plate is of "Gottlieb M.," a forty-two-year-old Jew from Vilnius, who likewise had been treated at many of the psychiatric clinics in Western Europe. Given the extraordinary movement of millions of Eastern Jews through Western Europe, beginning in the early 1880s, toward England and America, the appearance of these few cases of what comes to be called "Munchausen syndrome" should not surprise. Without any goal, these Jews "wandered" only in the sense that they were driven West, and that some should seek the solace of the clinic where they would at least be treated as individuals, even if sick individuals, should not make us wonder. What is striking is that Meige provides images and analyses that stress the pathognomonic physiognomy of the Jew—especially his eyes. The images gaze at us, informing us of their inherent hysterical pathology. The Jew is the hysteric; the Jew is the feminized Other; the Jew is seen as different, as diseased. This is the image of the hysteric with which the Jewish scientist was confronted. His "startle" effect was to see himself as the Other, as the diseased, but most important as the feminized Other, the altered form of his circumcised genitalia reflecting the form of that of the woman.
The "wandering Jew" as the model for the psychopathology of
the Eastern Jew. From Henry Meige, Étude sur certains
néuropathes voyageurs: Le juif-errant a la Salpêtrière
(Paris: L. Battaille et cie., 1893), p. 17.
(Bethesda, Md.: National Library of Medicine.)
No wonder that Jewish scientists such as Jacobs, Fishberg, and Freud—in very different ways—sought to find the hysteric outside of their own self-image. For that image was immutable within the biology of race. Fishberg quotes the accepted wisdom (in order to refute it for himself and project it onto the Eastern Jew) when he cites Richard An-
The image of "Moser C. called Moses," one of the modern "wandering Jews,"
gazes at the reader. From Henry Meige, Étude sur certains néuro-pathes
voyageurs: Le juif-errant a la Salpêtrièe (Paris: L. Battaille et cie., 1893), p. 25.
(Bethesda, Md.: National Library of Medicine.)
dree: "No other race but the Jews can be traced with such certainty backward for thousands of years, and no other race displays such a constancy of form, none resisted to such an extent the effects of time, as the Jews. Even when he adopts the language, dress, habits, and customs of the people among whom he lives, he still remains everywhere the same. All he adopts is but a cloak, under which the eternal Hebrew survives; he is the same in his facial features, in the structure of his body, his temperament, his character."[145] And this constancy of character, with its de-
The physiognomy and the gaze of "Gottlieb M.,"
a forty-two-year-old Jew from Vilna, "proves" the
psychopathology of the Jew. From Henry Meige,
Étude sur certains néuropathes voyageurs:
Le juif-errant a la Salpêtrière (Paris:
L. Battaille et cie., 1893), p. 29.
(Bethesda, Md.: National Library of Medicine.)
viant sexual nature, leads to the disease that marks the Jew, that leads to hysteria. Because the etiology of the Jew's hysteria, like the hysteria of the woman, was to be sought in "sexual excess."[146] Specifically in the "incestuous" inbreeding of this endogenous group: "Being very neurotic, consanguineous marriages among Jews cannot but be detrimental
to the progeny."[147] Jews (especially male Jews) are sexually different; they are hysterical and they look it.
The clinical gaze of the Jewish physician now becomes the object of the gaze of study. The image of the eyes attributed to the Jew reappears in the context of the science of race. It is this biological definition of all aspects of the Jew that helps form the fin-de-siècle idea of the Jew. The scientific gaze should be neutral. The scientific gaze should be beyond or above all of the vagaries of individual difference.[148] As George Herbert Mead put it: "Knowledge is never a mere contact of our organisms with other objects. It always takes on a universal character. If we know a thing, explain it, we always put it into a texture of uniformities. There must be some reason for it, some law expressed in it. That is the fundamental assumption of science."[149]
But race is but one of the categories of the visualization of the hysteric that played a role in shaping the image of the hysteric in the course of the nineteenth century. For the construction of seeing the hysteric took many different forms in providing a composite image of the hysteric, an image in bits and snatches, an image that revealed the "truth" about the hysteric's difference to him- or herself. The nosology of the "categories" of difference are really quite analogous to Charcot's construction of the visual pattern of the actions of the hysteric. One can argue that Freud's intellectual as well as analytic development in the 1890s was a movement away from the meaning of visual signs (a skill that he ascribes to Charcot in his obituary of 1893) and to the interpretation of verbal signs, from the crudity of seeing to the subtlety of hearing.[150] Charcot understands the realism of the image to transcend the crudity of the spoken word. In a letter to Freud on 23 November 1891 he commented concerning the transcription of his famed Tuesday lectures that "the stenographer is not a photographer."[151] The assumption of the inherent validity of the gaze and its mechanical reproduction forms the image of the hysteric. The central argument that can be brought is that this vocabulary of seeing remains embedded in Freud's act of understanding the hysteric, who must be seen to be understood. This is not present in the earliest papers on hysteria written directly under Charcot's influence, such as Freud's differential diagnosis of organic and hysterical paralysis written in 1886.[152] For Freud the rejection of Charcot's mode of seeing the hysteric is also a rejection of the special relationship that the Jew has with the disease. The theme of the specific, inherited risk of the Jew for hysteria (and other forms of mental illness) was reflected in the work of Charcot which Freud translated.[153] But even more so this general claim about the hereditary risk of the Jew was
linked to a diagnostic system rooted in belief in external appearance as the source of knowledge about the pathological. For the seeing of the Jew as different was a topos of the world in which Freud lived. Satirical caricatures were to be found throughout the German-speaking world, which stressed the Jew's physical difference, and in the work of Charcot (and his contemporaries) these representations took on pathological significance.
Indeed, Freud's purchase of a lithograph of Brouillet's painting of Charcot in August of 1889 can well be understood as a compensation of Freud's rejection of Charcot's mode of seeing and representing the hysteric. Indeed, it must also be understood as a compensation for his abandonment of his identification with the anti-Semitic Jean-Martin Charcot[154] —for whom Jews, as the essential "moderns," were at special risk as hysterics—and his new alliance with the provincial Jew Hippolyte Bernheim.[155] Such a movement parallels the abandonment of ideas of trauma—still for Charcot the cause of hysteria (in women as well as in Jews)—and its replacement with the etiology of hysteria in the psyche. As Freud states:
For [the physician] will be able to convince himself of the correctness of the assertions of the school of Nancy [Bernheim] at any time on his patients, whereas he is scarcely likely to find himself in a position to confirm from his own observation the phenomena described by Charcot as "major hypnotism," which seem only to occur in a few sufferers from grande hysterie .[156]
It is the scientific "observation," the gaze of the Jew rather than the gaze directed at the Jew, which marks the distinction between Charcot and Bernheim. Freud's conversion to Bernheim's mode of seeing the "usual" rather than seeing the "unique" also marks the beginning of his rejection of reducing the origin of hysteria to the single, traumatic event.
This returns us to the problem of defining the visual precursors for Charcot and for Freud. We must trace the image of the epileptic and the meaning of trauma—two clearly linked images in Freud's vocabulary of the hysteric—to see how Freud's reading of the hysteric is linked through these images of trauma to the central image of difference, the Eastern European Jews as hysterics (or perhaps more accurately, provincial Jews as parvenus, out of their minds because they are out of their natural place). It is the discourse on the relationship between trauma and hysteria that provides the key to Freud's—and many of his contemporaries'—ambivalence concerning models for therapy.
Trauma is not a neutral concept. There has been a general acceptance
of the historical model of the "railway spine," hysterical trauma resulting from railway accidents, as a means of understanding the traumatic nature of hysteria at the turn of the century.[157] Indeed, in much of the early work on hysteria these images haunt the literature. The hysteric is the sufferer from traumatic neurosis similar to that caused by experiencing a train accident, as outlined by Herbert Page in his classic work, Injuries of the Spine and Spinal Cord (1883), and accepted in toto by Charcot in his work on the neurosis of fright or shock. Both men and women are therefore equally at risk for such forms of psychopathology. Hysteria is thus merely the direct (brain or spinal cord lesion) or indirect (shock) result of trauma. And here the confusion between the models of hysteria evolved by Charcot and Hughlings Jackson must be stressed. For the traumatic event causes hysteria only in those who are predisposed to being hysteric (Charcot), but the lesion caused by trauma also releases those subterranean aspects of our earlier evolution held in check by the highest order of neurological organization (Hughlings Jackson). The Jew is predisposed to hysteria both because of hereditary and consanguinity (incestuous inbreeding) and, as we shall see, by the trauma of civilization as represented by the Jews' predisposition to the somatic diseases linked to hysteria, such as syphilis.
The fin-de-siècle image of trauma is one with modern civilization, with the train. As Sir Clifford Allbutt, Professor of Medicine at Cambridge University, stated in an essay in the Contemporary Review of 1895:
To turn now . . . to nervous disability, to hysteria . . . to the frightfulness, the melancholy, the unrest due to living at a high pressure, the world of the railway, the pelting of telegrams, the strife of business . . . surely, at any rate, these maladies or the causes of these maladies are more rife than they were in the days of our fathers? To this question . . . there is, I know, but one opinion on the subject in society, in the newspapers, in the books of philosophers, even in the journals and treatises of the medical profession.[158]
And thus the railroad, railway accidents, and the speed of modern life all collaborate to create the hysteric. But nineteenth-century "railway" medicine faced a dilemma that later faced Sigmund Freud. Trauma—such as involvement in a railway crash—is the cause of hysteria, but why do not all individuals who are involved in railway crashes become hysteric? This question was answered in part by the neurologist C. E. Brown-Séquard, who, as early as 1860, had argued that there were hereditary transmissions of acquired injuries, as in the case of "animals born of parents having been rendered epileptic by an injury to the spinal
cord."[159] This view quickly becomes a standard one in the literature on "railway spine."[160]
The image of the hysteric being at risk because of his or her inheritance limited the field from which the hysteric could be drawn. Thus the physician could, under most circumstances, see him- or herself as a separate category, as distanced from the hysteric as from the child of alcoholics or criminals. But not the Jewish physician. For the Jewish physician is at risk no matter which theory of hysteria one accepted.[161] Some views using the model of biological determinism had it that the Jew was at risk simply from inheritance; some views sought after a sociological explanation. But both views, no matter what the etiology, saw a resultant inability of the Jew to deal with the complexities of the modern world, as represented by the Rousseauean city. The trauma of "modern life" was closely linked to the image of the city. For nineteenth-century medicine (whether psychiatry or public health), cities are places of disease and the Jews are the quintessential city dwellers, the Americans of Europe. Richard Krafft-Ebing believed that civilization regularly brings forth degenerate forms of sexuality because of the "more stringent demands which circumstances make upon the nervous system," circumstances that manifest themselves in the "psychopathological or neuropathological conditions of the nation involved."[162] For him (and for most clinical psychiatrists at the turn of the century) the Jew is the ultimate "city person" whose sensibilities are dulled, whose sexuality is pathological, whose materialistic, money-grubbing goals are "American," whose life is without a center. It is also the city that triggers the weakness hidden within the corrupted individual. It is its turbulence, its excitement, what August Forel in The Sexual Question (1905) calls its "Americanism," that leads to illnesses such as hysteria:
Americanism.—By this term I designate an unhealthy feature of sexual life, common among the educated classes of the United States, and apparently originating in the greed for dollars, which is more prevalent in North America than anywhere else. I refer to the unnatural life which Americans lead, and more especially to its sexual aspect.[163]
This is an image seen by physicians of the period as "Jewish" in its dimensions. Jews manifest an "abnormally intensified sensuality and sexual excitement that lead to sexual errors that are of etiological significance."[164] Jewish scientists, when they address this question directly, seek for a developmental rather than a hereditary reason for this evident higher rate of hysteria. They seek out the two-thousand-year Diaspora as the origin of trauma.[165] But this does not free them. Given the views
of Brown-Séquard, there is really little escape no matter what the cause. The Jew becomes the hysteric and the hysteria is measured by the sexual abnormality of the Jew.
Thus when we turn to Freud's case studies, either in the collaborative Studies in Hysteria of 1895 or in his later and much more complex studies, such as his study of Dora (1905 [1901]), we face the question of Freud's (and Breuer's) representation of the Jew—of his "seeing" (or, perhaps better, "hearing") the Jew. In an earlier study I argued that the image of Anna O. in Breuer's case-study contribution to the Studies in Hysteria masked the "Jewishness" of Bertha Pappenheim.[166] In Freud's own contributions (such as the case of Katherina or Miss Lucy R.) there is the attempt to universalize the image of the hysteric through the citation—not of cases of male hysteria—but those of non-Jewish hysterics. But the common qualities ascribed to the hysteric and the Eastern, male Jew remain central to the representation of this nosological category for Freud.
This can be seen in a close reading of what has become the exemplary "case of hysteria" for our contemporary reading of the history of hysteria, Freud's case of Dora.[167] Seen by contemporary feminist critics, such as Hélène Cixous, as "the core example of the protesting force of women,"[168] it is also the classic example of the transmutation of images of gender and race (masculinity and "Jewishness") into the raceless image of the feminine. Freud used the case of Dora to argue not only for the necessary publication of case studies, but also for the needed masking of the analysand. The disguising of the identity of Dora is complete. There is no sign in the case study of the "racial" identity of Ida Bauer, the Eastern European Jewish daughter of Philip Bauer, whose syphilis was treated by Freud some six years before the beginning of Dora's analysis. Charcot (and Freud) had attempted to distance the diseases of syphilis and hysteria, and yet a relationship between the two patterns of illness remained. This omission, such as Josef Breuer's omission of his patient's "racial" identity in his narrative of Anna O.'s case, while including it in his case notes, masks a salient aspect of the case. We can best quote Freud in this regard, when he returns to the 1895 case of Katherina in 1924 and observes concerning his replacement of the relationship with the patient's father with the word "uncle": "Distortions like the one which I introduced in the present instance should be altogether avoided in reporting a case history."[169]
Perhaps as important for our reading of the suppressed aspects of the case of Dora (Ida Bauer) is the fact that her beloved brother Otto Bauer was one of the founders of the Austrian Socialist Party. His attitude toward his Jewish identity is of importance. For Austro-Marxism
advocated cultural-national autonomy for all people within the diverse Hapsburg Empire—except for the Jews. These Marxists saw assimilation as inevitable and positive, and they tied assimilation to a distinct distaste for Yiddish (and subsequently Hebrew) as linguistic signs of a negative separatism (a sign that took on positive meaning when ascribed to Czech or Hungarian as "national" languages). While Otto Bauer was an "Eastern Jew" himself, as he was born of Bohemian ancestry in Vienna, he was ambivalent about the idea of race. "Race" was an acceptable label for the other national groups, since it was associated by them with positive ideas of autonomy, but for the Jews (especially Eastern Jews) it was always a sign of the pathological.[170] Bertha Pappenheim, Breuer's Anna O., stated it quite baldly in an essay published at the turn of the century. Raised in an orthodox Jewish home, for her the German-language schools developed in the Eastern reaches of the Hapsburg Empire were "a stronghold, often conquered in battle, in the fight against the malaise from which Galician Jewry suffers as from a hereditary disease."[171] It is the cure of this hereditary disease that Freud undertakes in treating Dora (and thus treating an aspect of his own identity). This is, indeed, the hidden meaning of the development of the idea of transference and countertransference which is nascent in the case of Dora and why Freud's own understanding of this process is blocked in this case.
The centerpiece of Freud's study of Ida Bauer is, according to Freud's argument, the attempt to explain the origin of a case of hysteria through the analysis of the Oedipal triangle as perceived by a patient whose object of attraction is of the same sex. The complex relationships are between her father (Philip), her mother (Käthe), and Dora; the father's lover (Frau K.) and her husband (Herr K.), the attempted seducer of Dora, who has traditionally been the focus of the interpretation of the study. Much time and effort has been expended to understand Freud's complex misreading of this case. What is clear is that there are a number of misreadings by Freud in the text. Jacques Lacan pointed out one of the central ones: that the globus hystericus manifested by Dora is interpreted by Freud as the symbolic representation of orality within a specific context in the case study. The lover's seduction of the impotent father is described in Freud's analysis as an act of fellatio rather than being understood as cunnilingus.[172] This displacement is, however, not merely the shift of Freud's focus from the genitalia of the female to those of the male. Rather it is a double displacement—for the act of fellatio is also the emblematic act of male homosexual contact. What such a displacement means can be found if the "scientific" context of the meaning of the act of fellatio in the medical debates of the nineteenth
century are followed. Through such a contextualization we can outline Freud's understanding of the transmission of a "disease" (the collapse of language as represented by the symptom of the globus hystericus in Ida Bauer) as necessarily associated with the act of sucking a male's penis.
Let us begin with this misreading as a sign of Freud's representation of the idea of race in the guise of the representation of the feminine, as it replaces the male's genitalia as the object of attraction—and, therefore, sight—with the woman's. For Freud the act of seeing one's genitalia is one which is especially "feminine": "The pride taken by women in the appearance of their genitals is quite a special feature of their vanity; and the disorders of the genitals which they think calculated to inspire feelings of repugnance or even disgust have an incredible power of humiliating them, of lowering their self-esteem, and of making them irritable, sensitive, and distrustful."[173] The special quality of seeing the female's genitalia, genitalia normally understood by Freud as presence in the fantasy of their absence, points toward the other genitalia, the male genitalia, seen by the male, which when "disordered" points toward pathological nature of the male. But what is this disorder? In the case study it is, on one level, the origin of Ida Bauer's understanding about the diseased nature of her genitalia, the syphilitic infection of her father. One of the most interesting qualities ascribed to the father from the very beginning of the case study is the fact that he was syphilitic. The relationship between the physical trauma of syphilis and the image of the syphilitic is central to understanding the image of the hysteric which Freud evolves in his study. In the case of Dora's father, his "gravest illness . . . took the form of a confusional attack, followed by symptoms of paralysis and slight mental disturbance."[174] Freud diagnoses this as a case of "diffuse vascular affection; and since the patient admitted having had a specific infection before his marriage, I prescribed an energetic course of antiluetic treatment."[175] Four years later the father brings his daughter to Freud for treatment. Freud argues in a footnote for the retention of the relationship between the etiology of hysteria in the offspring and the syphilitic infection of the father. "Syphilis in the male parent is a very relevant factor in the etiology of the neuropathic constitution of children."[176] Here is the trauma—this case of hysteria is a form of hereditosyphilis transmitted by the father. Freud's emphasis on this line of inheritance is not solely because Ida Bauer's father had evidently (according to the account in the case study) infected her mother (and therefore his daughter), but because the general laws of the inheritance of disease which were accepted during this period argued that the son inherits the diseases of the mother (and therefore her father) while the daughter in-
herits the diseases of the father (and therefore his mother).[177] Freud later uncovers another sign of this biological predisposition in the fact that "she had masturbated in childhood."[178] This is the link that brings together the trauma (the syphilitic infection of the father), the mode of transmission (sexual intercourse with a circumcised penis), the Jewishness of the father as represented in his pathological sexuality, and the hysterical neurosis of the daughter. The merging of various forms of illness, from syphilis to hysteria, is through the model of inherited characteristics. The "real" disease is the degeneracy of the parent, and its manifestation in specific illness can vary from individual to individual.[179] Thus syphilis and hysteria are truly forms of the same pattern of illness.
One reading of the case would be to say that hypersexual Jewish males pass on their Jewish disease to their daughters in the form of hysteria. But this discourse is present in Freud's text only if we contextualize the meaning of syphilis within the context of Freud's self-definition as a Jew and that of his patient, Ida Bauer.
Freud creates very early on a differential diagnosis between tabes dorsalis (a label for one of the late manifestations of syphilis) and hysteria, at least when it appears in a woman who is infected with syphilis. He undertakes this in an extended footnote at the very beginning of the study in which he documents the central diagnostic thesis of this case study: that it is the ordered narrative of the patient about her illness which is disrupted in the hysteric. In other words, the hysteric lies: "The patient's inability to give an ordered history of their life insofar as it coincides with the history of their illness is not merely characteristic of the neurosis. It also possesses great theoretical significance."[180] The relationship between the sexual etiology of the hysteric and the hysteric's discourse represents the underlying shift from an image of race to one of gender (for as we shall see, the discourse of the Jew is a primary marker of difference). The counterexample is brought in Freud's notes, a case study of a patient who "had been for years . . . treated without success for hysteria (pains and defective gait)." She narrates her "story . . . perfectly clearly and connectedly in spite of the remarkable events it dealt with." Freud concludes this "could not be . . . [a case] of hysteria, and immediately instituted a careful physical examination. This led to the diagnosis of a fairly advanced stage of tabes, which later was treated with Hg injections (Ol. cinereum) by Professor Lang with markedly beneficial results."[181] Here the image of the "defective gait," which is one of the hallmarks of the "hysteric" in the nineteenth century (and the history created for this image at the Salpêtrière), recurs, only to be revealed
as the final stages of syphilis. The irony is that it is Joseph Babinski whose neurological work at the Salpêtrière provided the clue for such an analysis of the impaired plantar reflex[182] and Charcot himself, in his work on intermittent claudication, who provided the racial context for such impairment.[183] (And, indeed, there is a link of intermittent claudication to the image of the hysteric.)[184] In this case of Dora, it is revealed only at the very close of the case that one of Dora's primary symptoms was that "she had not been able to walk properly and dragged her right foot. . . . Even now her foot sometimes dragged."[185] Freud sees this "disorder, the dragging of one leg," as having a "secret and possibly sexual meaning of the clinical picture."[186] Freud interprets this as a sign of the "false step" that Dora had imaged herself to have taken during the attempted seduction by Herr K. at the lake. Later Felix Deutsch, who treated Ida Bauer after she broke off her analysis with Freud, observed with surprise that the "dragging of her foot, which Freud had observed when the patient was a girl, should have persisted twenty-five years."[187] This remained a central sign for her affliction, a sign that is not solely the association between the accident she had as a child and the bed rest that accompanied it. For the incapacity of gait is also a racial sign in Ida Bauer's Vienna and is associated with the "impairment" of the Jew. For it is the Jew, in a long Austrian tradition as old as the eighteenth century, who is at greatest risk in having both impaired gait[188] and syphilis. It is this image in the case of Dora that links the impairment of the syphilitic and the hidden image of the Jew.
The association of the syphilitic infection of the father and the neurosis of the daughter is linked by Freud in his analysis of the physical symptom of leukorrhea, or genital catarrh, an increased "disgust[ing] . . . secretion of the mucous membrane of the vagina."[189] Dora associates this with her lesbian "disgust" toward Herr K.'s attempted heterosexual seduction (in Freud's reading) and the feeling of his "erect member against her body."[190] Freud's conclusion is that for Ida Bauer "all men were like her father. But she thought her father suffered from venereal disease—for had he not handed it on to her and to her mother? She might therefore have imagined to herself that all men suffered from venereal disease, and naturally her conception of venereal disease was modelled upon her one experience of it—a personal one at that. To suffer from venereal disease, therefore, meant for her to be afflicted with a disgusting discharge."[191] Freud thus interprets one of two dreams narrated to him by Dora in terms of the connection among the "disgusting catarrh," the wetness of bed-wetting and masturbation, and her mother's compulsive cleanliness. "The two groups of ideas met in
Charcot's diagnostic category of intermittent claudication was used
as a marker for racial difference. From P. Olivier and A. Halipré, "Claudication
intermittente chez un homme hystérique atteint de pouls lent permanen," La
Normandie Médicale 11 (1896): 23.
(Bethesda, Md.: National Library of Medicine.)
this one thought: 'Mother got both things from father: the sexual wetness and the dirtying discharge.'"[192] In the recurrent dream the connection (right word) is made through the symbolic representation of the "drops," the jewels that her mother wishes to rescue from the fire that threatens the family.[193] Freud interprets the "drops"—the jewelry [Schmuck ]—as a switch-word, while "jewelry" [Schmuck ] was taken as an equivalent to "clean" and thus as a rather forced contrary of "dirtied."[194] Freud stresses that the "jewels" become a "jewelcase" in the dream and that this term (Schmuckkasten ) is "a term commonly used to describe female genitals that are immaculate and intact."[195]
One can add another layer of misreading. As I have shown, there is a subtext in the hidden language of the Jews. In Viennese urban dialect, borrowed from Yiddish, Schmock has another meaning. Schmock even in German urban ideolect had come to be the standard slang term for the male genitals. The hidden meaning of the language of the Jews is identical to the lying of the hysteric, the central symptom of hysteria, according to Freud. This transference can be seen in Freud's early description of the discourse of two Eastern male Jews in a letter to his friend Emil Fluss on the return trip from Freiburg to Vienna in 1872:
Now this Jew talked the same way as I had heard thousands of others talk before, even in Freiburg. His face seemed familiar—he was typical. So was the boy with whom he discussed religion. He was cut from the cloth from which fate makes swindlers when the time is ripe: cunning, mendacious, kept by his adoring relatives in the belief that he is a great talent, but unprincipled and without character. I have enough of this rabble.[196]
The misreading of the text is a repression of the discourse of the male Eastern Jew—the parvenu marked by his language and discourse as different and diseased. Hidden within the female genitalia (the Schmuckkasten ) is the image of the male Jew as represented by his genitalia (the Schmock ). The replacement of the "Jewish" penis—identifiable as circumcised and, as we shall see, as diseased, by the "German" vagina stands at the center of Freud's revision of the identity of Ida Bauer.
In my study Jewish Self-Hatred , I have extensively shown that an ancient Western tradition labels the language of the Jew as corrupt and corrupting, as the sign of the inherent difference of the Jew.[197] This tradition sees the Jew as inherently unable to have command of any "Western"—that is, cultural—language (indeed, even the "holy language," Hebrew). The Jew is not only "not of our blood," as Monsignor Joseph Frings of Cologne expressed it in 1942, but also "does not speak our language."[198] For the acculturated Eastern Jew in Vienna, mauscheln ,
the speaking of German with a Yiddish accent, intonation, or vocabulary, is the sign of this difference. And this is the language of Freud's mother, Amalia Freud née Nathanson, the invisible woman in all of his autobiographical accounts. As Freud's son Martin noted, she was a Galician Jew from Brody who remained a typical Polish Jew, "impatient, self-willed, sharp-witted and highly intelligent." She retained the language, manner, and beliefs of Galicia:
[She was] absolutely different from Jews who had lived in the West for some generations. . . . These Galician Jews had little grace and no manners; and their women were certainly not what we should call "ladies." They were highly emotional and easily carried away by their feelings. . . . They were not easy to live with, and grandmother, a true representative of her race, was no exception. She had great vitality and much impatience.[199]
It is in the image of the mother that the qualities ascribed to the hysteric, to Ida Bauer, can be found. In suppressing the shift of language, Freud also suppresses the "hidden" reference to the "Jewish" penis. The hidden discourse of the Jew, hidden within the high German culture discourse, is ignored.
This "misreading" of the female for the male organ is in truth a "misseeing" of the genitalia as Freud traces the origin of Ida Bauer's knowledge of the act of fellatio, the "seeing" as well as sucking of the male member. Freud understands this "so-called sexual perversion" as being "very widely diffused among the whole population, as everyone knows except medical writers upon the subject. Or, I should rather say, they know it too; only they take care to forget it at the moment when they take up their pens to write about it. So it is not to be wondered at that this hysterical girl of nineteen, who had heard of the occurrence of such a method of sexual intercourse (sucking at the male organ), should have developed an unconscious phantasy of this sort and should have given it expression by an irritation in her throat and by coughing."[200] Freud reports that Dora's governess, to whom she was evidently as attracted as she was to Frau K., "used to read every sort of book on sexual life and similar objects, and talked to the girl about them, at the same time asking her quite frankly not to mention their conversations to her parents, as one could never tell what line they might take about them."[201] But it is clear according to Ida Bauer's account that she did not only "hear" about such sexual activity but learned about it in quite another way. Later in the case study, after Freud had begun to explain the homosexual attraction which Dora felt for Frau K., this narrative shifts.
After Dora's father writes to Herr K. to demand an explanation of his actions toward his daughter, Herr K. "spoke of her with disparagement, and produced as his trump card the reflection that no girl who read such books and was interested in such things could have any title to a man's respect. Frau K. had betrayed her and had calumniated her; for it had only been with her that she had read Mantegazza and discussed forbidden topics."[202] It is the book, a foreign book, that "infects" her, and makes her "sick," that is, "hysteric." Like her governess, Frau K. had used her to get access to her father. This "error" in Freud's image of the etiology of hysteria is a displacement of the image of the infected and the infecting onto the world of high culture—not "German" high culture (Bildung ), of course, but the medical culture of the sexologist.
Paolo Mantegazza (1831-1901) was one of the standard ethnological sources for the late nineteenth century for the nature of human sexuality. His three-volume study of the physiology of love, the hygiene of love, and the anthropology of love was the standard popular introduction to the acceptable social discourse on sexuality in late nineteenth-century Europe.[203] His importance for Freud should not be underestimated. One of a group of physician-anthropologists (such as Cesare Lombroso), Mantegazza had pioneered the introduction of the study (and enjoyment) of Erthroxylon coca and its derivative, cocaine, in the late 1850s. Following the publication of Darwin's Descent of Man , Mantegazza became one of Darwin's most avid correspondents (and sources), supplying Darwin with a series of "anthropological" photographs that Darwin used for his later work.
Mantegazza's work, like that of Charcot, emphasized the "seeing" of difference, a view that is epitomized in Mantegazza's basic study of physiognomy and expression of 1885. But for late nineteenth-century science the controversial centerpiece of Mantegazza's work is his trilogy on love and sex: Fisiologia dell' amore (1872), Igiene dell' amore (1877), and Gli amori degli uomini (1885).[204] Cited widely by sexologists from Cesare Lombroso, Richard Krafft-Ebing, Havelock Ellis, and Iwan Bloch to Magnus Hirschfeld, Mantegazza remained one of the accessible, "popular" sources for scientific knowledge (and misinformation) for the educated public at the turn of the century. It is clear that Ida Bauer could have read (and probably did read) either Mantegazza or similar texts, whether under the tutelage of her companion or on her own initiative. What is of interest is how Freud reads this contradiction in her account: Did she read them, or only hear about their content? What is inherently dangerous about Mantegazza from the standpoint of Freud's refusal to relate to the accusation that Ida Bauer had read him? If we turn to
the trilogy, it is clear (and Madelon Spregnether agrees[205] ) that the text that best fits the pejorative description of Herr K. is the final text in this series, on the anthropology of sexuality.[206] There one finds an extended discussion of "the perversions of love," including "mutual onanism," "lesbianism and tribadism," as well as "histories" of these practices. (However, there are similar discussions in the seventh chapter of Mantegazza's study on the "hygiene of love," which details the "errors of the sexual drive.")
Now this is clearly what Freud should have understood—given his reading—as of importance to Ida Bauer, but what in this volume would have been of importance to Sigmund Freud? If we turn to the chapter after the one on "perversions," we come to a detailed discussion of the "mutilation of the genitals," which recounts the history of these practices among "savage tribes" including the Jews. Indeed, it is only in Mantegazza's discussion of the Jews that the text turns from a titillating account of "unnatural practices" into an Enlightenment polemic against the perverse practices of that people out of their correct "space" and "time"—the Jews:
Circumcision is a shame and an infamy; and I, who am not in the least anti-Semitic, who indeed have much esteem for the Israelites, I who demand of no living soul a profession of religious faith, insisting only upon the brotherhood of soap and water and of honesty, I shout and shall continue to shout at the Hebrews, until my last breath: Cease mutilating yourselves: cease imprinting upon your flesh an odious brand to distinguish you from other men; until you do this, you cannot pretend to be our equal. As it is, you, of your own accord, with the branding iron, from the first days of your lives, proceed to proclaim yourselves a race apart, one that cannot, and does not care to, mix with ours.
It is circumcision that sets the (male) Jew apart. In his dissertation of 1897 Armand-Louis-Joseph Béraud notes that the Jews needed to circumcise their young males because of their inherently unhygienic nature, but also because the "climate in which they dwelt" otherwise encouraged the transmission of syphilis.[207] The Jew in the Diaspora is out of time (having forgotten to vanish like the other ancient peoples); is out of correct space (where circumcision had validity). His Jewishness (as well as his disease) is inscribed on his penis.
But what does circumcision mean for a Viennese Jewish scientist at the end of the 1800s? The debates within and without the Jewish communities concerning the nature and implication of circumcision surfaced again in Germany during the 1840s. German Jews had become
acculturated into German middle-class values and had come to question the absolute requirement of circumcision as a sign of their Jewish identity. Led by the radical reform rabbi Samuel Holdheim in Germany and responding to a Christian tradition that denigrated circumcision, the debate was carried out as much in the scientific press as in the religious one.[208] There were four "traditional" views of the "meaning" of circumcision since the rise of Christianity. Following the writings of Paul, the first saw circumcision as inherently symbolic and, therefore, no longer valid after the rise of Christianity (this view was espoused by Eusebius and Origen); the second saw circumcision as a form of medical prophylaxis (as in the writing of Philo but also in the work of the central German commentator of the eighteenth century, Johann David Michaelis); the third saw it as a sign of a political identity (as in the work of the early eighteenth-century theologian Johann Spencer); the fourth saw it as a remnant of the early Jewish idol or phallus worship (as in the work of the antiquarian Georg Friedrich Daumer—this view reappears quite often in the literature on Jewish ritual murder).
In the medical literature of the time, two of these views dominated. They were the views that bracketed the images of "health" and "disease." These views saw circumcision either as the source of disease or as a prophylaxis against disease—and in both cases syphilis and masturbation, the two "diseases" that dominate the case of Dora, play a major role. Mantegazza notes that "the hygienic value of circumcision has been exaggerated by the historians of Judaism. It is true enough that the circumcised are a little less disposed to masturbation and to venereal infection; but every day, we do have Jewish masturbators and Jewish syphilitics. Circumcision is a mark of racial distinction; . . . it is a sanguinary protest against universal brotherhood; and if it be true that Christ was circumcised, it is likewise true that he protested on the cross against any symbol which would tend to part men asunder." The opposing view of circumcision in the scientific literature of the time saw circumcision as a mode of prevention that precluded the transmission of sexually transmitted diseases because of the increased capacity for "cleanliness."[209] It is classified as an aspect of "hygiene," the favorite word to critique or support the practice. (This view is closely associated with the therapeutic use of circumcision throughout the nineteenth century as a means of "curing" the diseases caused by masturbation, with, of course a similar split in the idea of efficacy: circumcision was either a cure for masturbation, as it eliminated the stimulation of the prepuce and deadened the sensitivity of the penis, or it was the source of Jewish male hypersexuality.)
A detailed medical literature links the very act of circumcision with
the transmission of syphilis, so that the prophylaxis becomes the source of infection. The literature that discusses the transmission of syphilis to newly circumcised infants through the ritual of metsitsah , the sucking on the penis by the mohel , the ritual circumciser, in order to staunch the bleeding, is extensive and detailed.[210]
The metsitsah was understood by the scientific community of the nineteenth century as a "pathological" one, as it was labeled as the source of the transmission of disease from the adult male to the male child. In the establishment of the Viennese Jewish community during the course of the early nineteenth century the debate on the abolition of circumcision was heard as loudly as anywhere else in Central Europe. Isaac Noah Mannheimer, the rabbi of the Seitenstettengasse synagogue and the de facto "chief rabbi" of Vienna (although this title did not officially exist), while a follower of Reformed Judaism, opposed the more radical "reforms" of theologians such as Samuel Holdheim. He strongly advocated the retention of Hebrew as the language of prayer (even though he had preached in Danish during his tenure in Copenhagen) and opposed mixed marriages and the abolition of circumcision. (The link among these three central issues in the self-definition of Viennese Jewry at mid-century should be stressed.) While no compromise was found on the first two issues (Hebrew was maintained as the language of the liturgy and mixed marriages were not authorized), a striking compromise was found in the third case. Together with Rabbi Lazar Horowitz, the spiritual leader of the orthodox community in Vienna, they abolished the practice of the metsitsah .[211] Although Horowitz was a follower of the ultraorthodox Pressburg Rabbi Moses Sofer, the abolition of the metsitsah became a marker between the practices of Viennese Jewry (which did not permit it for "hygienic" reasons) and the tradition of Eastern Jewry, such as the Jews of Pressburg and Freiburg (where Freud was circumcised).
Here is the link between the emphasis on fellatio in Freud's reading of the case of Dora and the syphilis that haunts the image of the (male) Jew in the case. It is the male sucking the penis of a male in the act of circumcision. Especially in the Viennese debates concerning the retention or abolition of circumcision, this "act" played a special role. For Freud the act of fellatio would be a sign not only of "perversion" but also of the transmission of disease; it would also be a sign that incorporated his own relationship between his racial identity with his coreligionists and, indeed, with other male authority figures. Thus the act of the female sucking on the penis of the male, a "pathological" act as it represents the spread of disease (hysteria) to the daughter, is a sub-
limation of the act of the male sucking on the penis of the male and spreading another disease, syphilis. It also represents, in the period during which Freud was writing and rewriting the case of Dora, Freud's own articulation of the end of his "homosexual" (i.e., homoerotic) relationship with Wilhelm Fliess, whose theories about the relationship between the nose and the penis are echoed in this case study as well as elsewhere in the fin-de-siècle work of Freud.[212]
But reading Mantegazza, we can go one step farther in our analysis of Freud's understanding of the meaning of sexually transmitted disease and its relationship to hysteria. For Mantegazza introduces his discussion of the exclusivity of the Jews with the following discussion:
It is altogether likely that the most important reason that has led men of various ages and of varying civilizations to adopt the custom of cutting off the prepuce has been that it was felt to be necessary to imprint upon the human body a clear and indelible sign that would serve to distinguish one people from another and, by putting a seal of consecration upon nationality, would tend to impede the mixture of races. A woman, before accepting the embraces of a man, must first make sure, with her eyes and with her hands, as to whether he was of the circumcised or the uncircumcised; nor would she be able to find any excuse for mingling her own blood-stream with that of the foreigner. It had, however, not occurred to the legislator that this same indelible characteristic would inspire in the woman a curiosity to see and to handle men of a different sort.
The seduction of the Jewish woman by the Other—whether the non-Jew or the lesbian—is the result of the "seeing" of the difference in the form of the genitalia. The need to "see" and "touch" the Other is the fault of the circumcised (male) Jew, whose very physical form tempts the female to explore the Other. Here we have another form of the displacement of the act of touching (sexual contact) with the permitted (indeed, necessary) act of seeing, but given a pathological interpretation. The rejection of mixed marriage and conversion by even "godless" Jews such as Sigmund Freud at this time is a sign of the need to understand the separateness of the Jew as having a positive valence. The labeling of converts as "sick" becomes a widely used fin-de-siècle trope.[213]
Ida Bauer's act of seeing her father is the act of seeing the (male) Jew. Central to the definition of the Jew—here to be understood always as the "male" Jew—is the image of the male Jew's circumcised penis as impaired, damaged, or incomplete and therefore threatening. The literature on syphilis—which certainly played a role in Freud's understanding of her father's illness as well as that of the daughter—contains a substantial discussion of the special relationship of Jews to the transmission and
meaning of syphilis. For it is not only in the act of circumcision that this association is made—it is in the general risk of the Jews as the carriers of syphilis and the generalized fear that such disease would undermine the strength of the body politic. Central to the case of Ida Bauer is a subtext about the nature of Jews, about the transmission of syphilis, and about the act of circumcision.[214] Both are associated with the image of the hysteric. It is Jewishness that is the central category of racial difference for the German reader and writer of the turn of the century.[215]
For the Jew in European science and popular thought was closely related to the spread and incidence of syphilis. Such views had two readings. The first model saw the Jews as the carriers of sexually transmitted diseases who transmitted them to the rest of the world. And their location is the city—Vienna. Here the link between the idea of the Jew as city dweller, as the disease that lurks within the confinement of the urban environment, becomes manifest. The source of the hysteria of the city is the diseased sexuality of the Jew. This view is to be found in Adolf Hitler's discussion of syphilis in turn-of-the-century Vienna in Mein Kampf (1925). There he (like his Viennese compatriot Bertha Pappenheim[216] ) links it to the Jew, the prostitute, and the power of money:
Particularly with regard to syphilis, the attitude of the nation and the state can only be designated as total capitulation. . . . The invention of a remedy of questionable character and its commercial exploitation can no longer help much against this plague. . . . The cause lies, primarily, in our prostitution of love. . . . This Jewification of our spiritual life and mammonization of our mating instinct will sooner or later destroy our entire offspring.[217]
Hitler's views also linked Jews with prostitutes and the spread of infection. Jews were the archpimps—Jews ran the brothels—but Jews also infected their prostitutes and caused the weakening of the German national fiber.[218] But also, Jews are associated with the false promise of a medical cure separate from the social cures that Hitler wishes to see imposed—isolation and separation of the syphilitic and his or her Jewish source from the body politic. Hitler's reference is to the belief that especially the specialty of dermatology and syphilology was dominated by Jews, who used their medical status to sell quack cures.
The second model that associated Jews and syphilis seemed to postulate exactly the opposite—that Jews had a statistically lower rate of syphilitic infection—because they had become immune to it through centuries of exposure. In the medical literature of the period, reaching across all of European medicine, it was assumed that Jews had a notably
lower rate of infection. In a study of the incidence of tertiary lues in the Crimea undertaken between 1904 and 1929, the Jews had the lowest consistent rate of infection.[219] In an eighteen-year longitudinal study H. Budel demonstrated the extraordinarily low rate of tertiary lues among Jews in Estonia during the prewar period.[220] All these studies assumed that biological difference as well as the social difference of the Jews were at the root of their seeming immunity.
Jewish scientists also had to explain the statistical fact of their immunity to syphilis. In a study of the rate of tertiary lues, the final stage of the syphilitic infection, undertaken during World War I, the Jewish physician Max Sichel responded to the general view of the relative lower incidence of infection among Jews as resulting from the sexual difference of the Jews.[221] He responds—out of necessity—with a social argument. The Jews, according to Sichel, show lower incidence not only because of their early marriage and the patriarchal structure of the Jewish family, but also because of their much lower rate of alcoholism. They were, therefore, according to the implicit argument, more rarely exposed to the infection of prostitutes, whose attractiveness was always associated with the greater loss of sexual control in the male attributed to inebriety. The relationship between these two "social" diseases is made into a cause for the higher incidence among other Europeans. The Jews, because they are less likely to drink heavily, are less likely to be exposed to both the debilitating effects of alcohol (which increase the risk for tertiary lues) as well as the occasion for infection. In 1927 H. Strauss looked at the incidences of syphilitic infection in his hospital in Berlin in order not only to demonstrate whether the Jews had a lower incidence but also to see (as in the infamous Tuskegee experiments among blacks in the United States) whether they had "milder" forms of the disease because of their life-style or background.[222] He found that Jews had indeed a much lower incidence of syphilis (while having an extraordinarily higher rate of hysteria) than the non-Jewish control. He proposes that the disease may well have a different course in Jews than in non-Jews. The marker for such a view of the heightened susceptibility or resistance to syphilis is the basic sign of difference of the Jews, the circumcised phallus.
The need to "see" and "label" the Jew at a time when Jews were becoming more and more assimilated and therefore "invisible" in Germany made the association with socially stigmatizing diseases that bore specific visible "signs and symptoms" especially appropriate. Mantegazza's view links the act of "seeing" the Jew sexually with the defamed practice of circumcision. In the German empire of the late nineteenth century all of the arguments placed the Jew in a special relationship to
syphilis and, therefore, in a very special relationship to the healthy body politic that needed to make the Jew visible. (The central medical paradigm for the establishment of the healthy state was the public health model that evolved specifically to combat the evils of sexually transmitted disease through social control.) Western Jews had been completely acculturated by the end of the nineteenth century and thus bore no external signs of difference (unique clothing, group language, group-specific hair and/or beard style). They had to bear the stigma of this special relationship to their diseased nature literally on the skin, where it could be seen. Not only on the penis where (because of social practice) it could be "seen" only in the sexual act. And then, because of the gradual abandonment of circumcision, be "seen" not to exist at all!
Just as the hysteric is constructed out of the perceived ability to categorize and classify categories of difference visually, the syphilitic Jew has his illness written on his skin. The skin of the hysteric, like the physiognomy of the hysteric, reflects the essence of the disease. Thus the skin becomes a veritable canvas onto which the illness of the hysteric is mapped. Seeing the hysteric means reading the signs and symptoms (the stigmata diaboli ) of the disease and representing the disease in a manner that captures its essence. It is the reduction of the ambiguous and fleeting signs of the constructed illness of the hysteric (constructed by the very nature of the definition of the disease in the nineteenth century). If the idea of the hysteric is tied to the idea of the feminization of the healthy Aryan male, or his "Jewification" (to use one of Hitler's favorite terms), then the representation of the disease must be in terms of models of illness that are convertible into the images of the feminized male. But these images of feminization are also tied to other, salient, fin-de-siècle images of race. For Jews bear the salient stigma of the black skin of the syphilitic, the syphilitic rupia .
The Jews are black, according to nineteenth-century racial science, because they are "a mongrel race which always retains this mongrel character." That is Houston Stewart Chamberlain arguing against the "pure" nature of the Jewish race.[223] Jews had "hybridized" with blacks in Alexandrian exile. They are, in an ironic review of Chamberlain's work by Nathan Birnbaum, the Viennese-Jewish activist who coined the word Zionist , a "bastard" race the origin of which was caused by their incestuousness, their sexual selectivity.[224] But the Jews were also seen as black. Adam Gurowski, a Polish noble, "took every light-colored mulatto for a Jew" when he first arrived in the United States in the 1850s.[225] Jews are black because they are different, because their sexuality is different, because their sexual pathology is written upon their skin. Gurowski's
"German-Jewish" contemporary, Karl Marx, associates leprosy, Jews, and syphilis in his description of his archrival Ferdinand Lassalle (in 1861): "Lazarus the leper, is the prototype of the Jews and of Lazarus-Lassalle. But in our Lazarus, the leprosy lies in the brain. His illness was originally a badly cured case of syphilis."[226] The pathognomonic sign of the Jew is written on the skin; it is evident for all to see.
The pathological image of the Jew was part of the general cultural vocabulary of Germany. Hitler used this image over and over in Mein Kampf in describing the Jew's role in German culture: "If you cut even cautiously into such an abscess, you found, like a maggot in a rotting body, often dazzled by the sudden light—a kike! . . . This was pestilence, spiritual pestilence, worse than the Black Death of olden times, and the people were being infected by it."
"Plague" (Seuche ) and pestilence (Pestilenz )—a disease from without, which, like syphilis, rots the body—was the model used to see the role of the Jew. The syphilitic weakening of the racially pure Germans by the Jews was likened by Hitler to the corruption of the blood of the race through another form of "mammonization," interracial marriage:
Here we have before us the results of procreation based partly on purely social compulsion and partly on financial grounds. This one leads to a general weakening, the other to a poisoning of the blood, since every department store Jewess is considered fit to augment the offspring of His Highness—and indeed the offspring look it. In both cases complete degeneration is the consequence.
If the Germans (Aryans) are a "pure" race—and that is for turn-of-the-century science a positive quality—then the Jews cannot be a "pure" race. Their status as a mixed race became exemplified in the icon of the Mischling during the 1930s. The Jewishness of the Mischling , to use the term from racial science that is parallel to "bastard" (the offspring of a "Black" and a "White" "race"), "looks" and sounds degenerate. They can have "Jewish-Negroid" [jüdisch-negroid ] features.[227] And this is often associated with their facile use of language, "the use of innumerable foreign words and newly created words to enrich the German language in sharp contrast to the necessary simplicity of the language of Germanic students."[228] The Jew's language reflects only the corruption of the Jew and his or her discourse. It is the sign of the "pathological early development" of the Mischling , who, as an adult, is unable to fulfill the promise of the member of a pure race. The weakness, but also the degenerate facility, of the Mischling is analogous to the image of the offspring of the syphilitic. And thus we come full circle. For the Jew is contaminated
by hysteria, whether it is the result of the trauma of infection or of heredity. And this weakness of the race is hidden within the corrupted (and corrupting) individual. Thus Hitler's image of the Mischling is on the offspring of a "Jewish" mother and an "Aryan" father—hidden within the name and Germanic lineage of the child is the true corruption of the race, the maternal lineage of the Jew. And as Jews claimed their lineage through the mother (rather than through the father as in German law) the Mischling becomes the exemplary hidden Jew just waiting to corrupt the body politic.
The image of the Mischling , the person impaired because of his or her heritage, brings us back full circle to the world of Ida Bauer. For here we have all of these themes of Jewish disposition and racial diagnosis summarized. The images that haunt Freud's representation of Ida Bauer—her language, the sexual acts of her imagination, their source, the relationship between pathology and infection—are all "racially" marked (at least notionally) in turn-of-the-century medical culture. For Freud, abandoning the act of seeing, an act made canonical in the work of his anti-Semitic mentor Charcot, is an abandonment of the associations of sight within this discourse of sexual difference. The case of Dora is an example of the power over language, of Freud's control over the language of his text, which reveals him not to be an Eastern Jew. Like his critique of the bad Greek of his critics when he held his first talk on male hysteria in Vienna, Freud is the master of the discourse of science and culture. Freud is a scientist who uses language as a scientist. In introducing the question of the nature of Ida Bauer's attraction to Frau K. he remarks: "I must now turn to consider a further complication, to which I should certainly give no space if I were a man of letters engaged upon the creation of a mental state like this for a short story, instead of being a medical man engaged upon its dissection." The act of writing the story is the sign of his special control of a "neutral" language, one that, as we have shown, is hardly neutral when it comes to placing Freud, the Eastern male Jew, at its center of risk. The meaning of the act of seeing for the Jewish physician shows the inherent truth of Robert Reininger's claim that "Unser Weltbild ist immer zugleich ein Wertbild,"[229] that we construct our understanding of the world from our internalized system of values.